Knowledge of the anatomy of this region is extremely important in determining the surgical approach in craniovertebral junction pathologies and tumors. Therefore, the distance of the tuberculum pharyngeum (TP), which is located in the center of this region, to other close and significant anatomical structures is important. This study was conducted using a total of 64 craniums. The width of the pars basilaris at the level of the TP and the distance from the TP to anatomical formations such as opisthion, basion, protuberentia occipitalis externa, condylus occipitalis, canalis caroticus, processus styloideus, foramen stylomastoideum, processus mastoideus and ala vomeris were measured. The difference in measurements between sexes and sides were evaluated. The distances from the TP to opisthion, protuberentia occipitalis externa, condylus occipitalis, left canalis caroticus, proccesus styloideus, foramen stylomastoideum and proccesus mastoideus were statistically higher in males than in females. On the other hand, no significant difference was observed between the sexes in the width of the pars basilaris at the level of the TP and in the distance between the TP to the basion, right canalis caroticus and ala vomeris. There was no statistically significant difference between the distances from TP to condylus occipitalis, canalis caroticus, proccesus styloideus, foramen stylomastoideum, proccesus mastoideus and ala vomeris in both sides and both sexes. In male and female anatomical struc craniums, the pars basilaris ossis occipitalis placed between the vomer and foramen magnum are similar in size. Although the distance of TP to important tures was significantly higher in males than in females, it was observed that the distances of TP to the right and left anatomical structures were symmetrical in all craniums. We think that knowledge of the cranium base morphometry and its bilateral symmetry will guide the interventions to be made here by taking the opposite side as a model.
The anatomic study of extracranial structures related to tuberculum pharyngeum
Nazli G. Ceri1, Ayse G. Sahmelikoglu1, Fulden Cantas2, Gizem Sakalli1
1 Department of Anatomy, Faculty of Medicine, Aydin Adnan Menderes University, Aydin, Turkey
2 Department of Biostatistics, Faculty of Medicine, Aydin Adnan Menderes University, Aydin, Turkey
SUMMARY
Sign up or Login
INTRODUCTION
Tuberculum pharyngeum (TP), which gives attachment to the pharyngeal raphe, the highest attachment of the superior pharyngeal constrictor, is a small elevation found on the midline of the pars basilaris ossis occipitalis (the basilar part of the occipital bone) (Standring, 2016). On the extracranial surface, the pharyngeal tubercle is located in the midline around the junction of the middle and lower clivus. There may be a small bone rise between the TP and the anterior margin of the foramen magnum, and this structure is called the crista pharyngea, but it is a very rare occurrence (Hofmann and Prescher, 2012).
The base of the cranium provides the support and protection of vital organs such as the brain and cerebellum, as well as forming the transition point of important vascular and neural structures located between the cranium and the upper cervical region. (Sharma and Garud, 2011). Trauma-induced disorders, tumors, vascular system diseases and degenerative diseases are frequently seen at the craniocervical junction, and treatment for these lesions are usually surgical (Zhong et al., 2018; Patel et al., 2016). Surgical approaches such as transoral-transpharyngeal directly reach the ventral midline of the basis cranii externa, and at the same time prevent damage to some important anatomical structures such as the sixth through the twelfth cranial nerves, internal carotid artery, internal jugular vein, inferior petrosal sinus, and inferior petroclival vein located in this region. These approaches afford direct and relatively safe avenues with few vital neurovascular structures in the midline plane. In lesions that require a posterior approach, the distance between the TP and the surrounding structures is surgically important (Wang et al., 2016; Hitotsumatsu et al., 1999; Patel et al., 2016).
In this study, we measured the distance between the TP and other anatomical formations, so as to determine the surgical confidence interval and to prevent damage during the surgical treatment of lesions or tumors that will occur in this area. In addition to radiological studies in this area, measurements obtained from studies on dry bones will provide healthier results and guide the surgeons.
MATERIALS AND METHODS
This study was conducted using a total of 64 randomly selected adult craniums (22 female and 42 male) without any structural deformities obtained from the bone archive in the Department of Anatomy, Faculty of Medicine, Aydin Adnan Menderes University. Measurement of the closest distance from the TP (Fig. 1, Table 1), as the main point of reference, to important structures were made with the help of an electronic clip. At the beginning of the study, 10 randomly selected craniums were independently evaluated by two observers. A day later, the same measurements were repeated and the intra-observation reliability was evaluated.
Statistical analysis
Whether or not quantitative variables conform with normal distribution was examined using the Kolmogorov-Smirnov test. Groups were compared by using two-independent samples t- tests for normally distributed variables and Mann Whitney U test for variables that did not show normal distribution. Dependent variables with normal distribution were compared with paired t test, and non-normally distributed dependent variable were compared with Wilcoxon T test. Statistically, p <0.05 values were considered significant.
RESULTS
In the study, the distance of the TP to 9 important anatomical structures and the pars basilaris width were evaluated using 64 craniums of known sexes (Fig. 1, Table 1).
In Table 2, the distances from the TP to opisthion, protuberentia occipitalis externa, condylus occipitalis, left canalis caroticus, proccesus styloideus, foramen stylomastoideum and proccesus mastoideus were statistically higher in males than in females. On the other hand, no significant difference was observed between the sexes in the width of the pars basilaris at the level of the TP and in the distance between the TP to the basion, right canalis caroticus and ala vomeris.
In Tables 3 and 4, there was no statistically significant difference between the distances from TP to condylus occipitalis, canalis caroticus, proccesus styloideus, foramen stylomastoideum, proccesus mastoideus and ala vomeris in both sides and both sexes.
DISCUSSION
For surgeons and clinicians, the structures in the basis cranii externa are very important. There are also studies evaluating clivus and condylus occipitalis morphometrically (Kızılkanat et al., 2006; Ozer et al., 2011; Ji et al., 2012). There are studies investigating the structure of basis cranii not only in the bone tissue in that region, but also in connective tissue and its properties related to membranous structures (Krmpotić-Nemanić et al., 2006; Aparna et al., 2019). As a matter of fact, even the distance of fossa navicularis, which is a rare variation on craniums, to TP has been measured (Cankal et al., 2004). TP is the central point of the nasopharynx and together with the anatomical structures adjacent to it, it is important in both breathing and swallowing (Krmpotić-Nemanić et al., 2006; Aparna et al., 2019). Despite the importance of the region, the insufficient number of studies led us to evaluate this area in morphometric detail.
In a study conducted in Croatia, Krmpotić-Nemanić et al. (2006) evaluated the distance of osseous epipharynx to anatomical formations in 60 basis cranii externa. Similar to our study, they measured the distance of the TP to ala vomeris, the basion, and the pars basilaris width at the level of the tuberculum pharyngeum. They did not observe any significant sex-related difference and reported the data only by age distribution. Likewise, we did not detect any significant difference between the sexes in these three parameters. In addition, they recorded the distance between the TP and the basion as 8.6±2.0 mm, the width in the pars basilaris as 26.8±5.5 mm and the distance between the ala vomeris as 17.27±3.8 mm. In our study, the distance between the TP and the basion was 12.58±1.40 mm in males and 11.97±1.27 mm in females, the width of the pars basilaris was 24.92±2.72 mm in male and 24.11±2.72 mm for female and the distance from both sides of ala vomeris was 17.60±2.17 mm for the right-side and 17.49±2.15 mm on the left-side in males, and 18.50±1.55 mm on the right-side and 18.50±1.41 mm on the left-side in females. We thought that the reason for the difference in the values obtained might be due to the difference based on population and sex.
A study (Erdem et al., 2018) where twenty-six adult dry skulls were measured reported that the distance between TP and canalis caroticus was 26.7±2.00 mm on the left-side and 27.5±2.22 mm on the right-side, while the distance between condylus occipitalis was 16.4±1.59 mm on the left-side and 16.3±1.79 mm on the right-side.
In our study, we determined that the distance between the TP and condylus occipitalis on the right-side was 16.76±1.70 mm in males and 15.38±1.65 mm in females, on the left-side was 16.97±2.82 in males and 15.28±1.40 mm in females; the distance between the TP and the canalis caroticus on the right-side was 31.80±2.19 mm in males and 31.60±2,79 mm in females, on the left was 31.81±2.16 mm in males and 30.27±1.44 mm in females. There is no significant difference between the sides in these studies. While they did not discriminate sex for these measurements in their studies, we found a significant difference between sexes.
In contrast to Zhong et al. (2018) who, without sex discrimination, found the distance between the TP and opisthion as 10.23±0.55 mm in the measurements on the basis cranii externa made on CT, our study found that this distance was 46.34±6.83 mm in males and 44.68±2.85 mm in females and that it was statistically significantly lower in females.
Ji et al. (2012) performed a radiological study on 40 craniums, and found that the distance to the anterior part of the condylus occipitalis was 15.65±1.65 mm on the left-side and 15.60±1.91 mm on the right-side and the distance of the TP to the canalis caroticus was 24.26±2.05 mm on the left-side, 26.25±2.26 mm on the right-side. In our study, we determined that the distance of the TP to the condylus occipitalis to the anterior part as 16.76±1.70 mm on the right-side, 16.97±2.82 mm on the left-side for males, 15.38±1.65 mm on the right-side and 15.28±1.40 mm on the left-side for females; the distance of the TP to the canalis caroticus was 31.80±2.19 mm on the right-side and 31.81±2.16 mm on the left-side for males, and 31.60±2.79 mm on the right-side and 30.27±1.44 mm in the left-side for females. Our study differs from those similar studies, as they did not separate the sexes of bones and there is difference in measurement methods used.
In Turkey, Aktas et al. (2013)’s study on cadavers identified the distance between the pharyngeal tubercle with arteria carotis interna as 38.95±4.67 mm. Since we used dry craniums in our study, we measured the distance of the TP to the canalis caroticus. We determined this distance as 31.80±2.19 mm on the right-side and 31.81±2.16 mm on the left-side for male, 31.60±2.79 mm on the right-side and 30.27±1.44 mm on the left-side for females. We think that morphometric studies performed on soft tissues affect the measurement values.
Although there are many studies on facial asymmetry (Al-Rudainy et al., 2019; Taylor et al., 2014; Sasaki et al., 2020; Linden et al., 2018), studies evaluating neurocranial asymmetry are almost nonexistent. Tuberculum pharyngeum, which is located in the center of the region where surgical interventions are frequently performed is surrounded by structures that are of vital importance. The fact that these important structures are at a similar distance on both sides of this point will increase the confidence interval of the interventions to be made by taking the opposite side as a reference.
CONCLUSION
The part of the occipital bone between the vomer and foramen magnum is similar in size in the male and female craniums. When the TP reference point was taken, it was seen that the distance to the anatomical structures was statistically longer in males, but it was symmetrical in all craniums. Knowing the distance of the tuberculum pharnygeum to many important anatomical structures will provide morphometric data for surgical interventions performed in this region. We think that morphometric studies of bone are anthropologically and surgically important.
Related articles


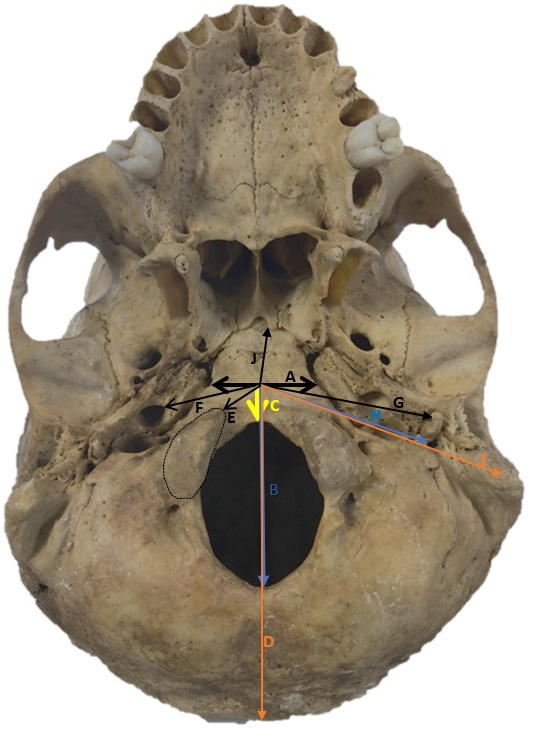 Fig. 1.- The location of the measurements in Table 1 in the basis cranii externa (Bone archive of Department of Anatomy).
Fig. 1.- The location of the measurements in Table 1 in the basis cranii externa (Bone archive of Department of Anatomy).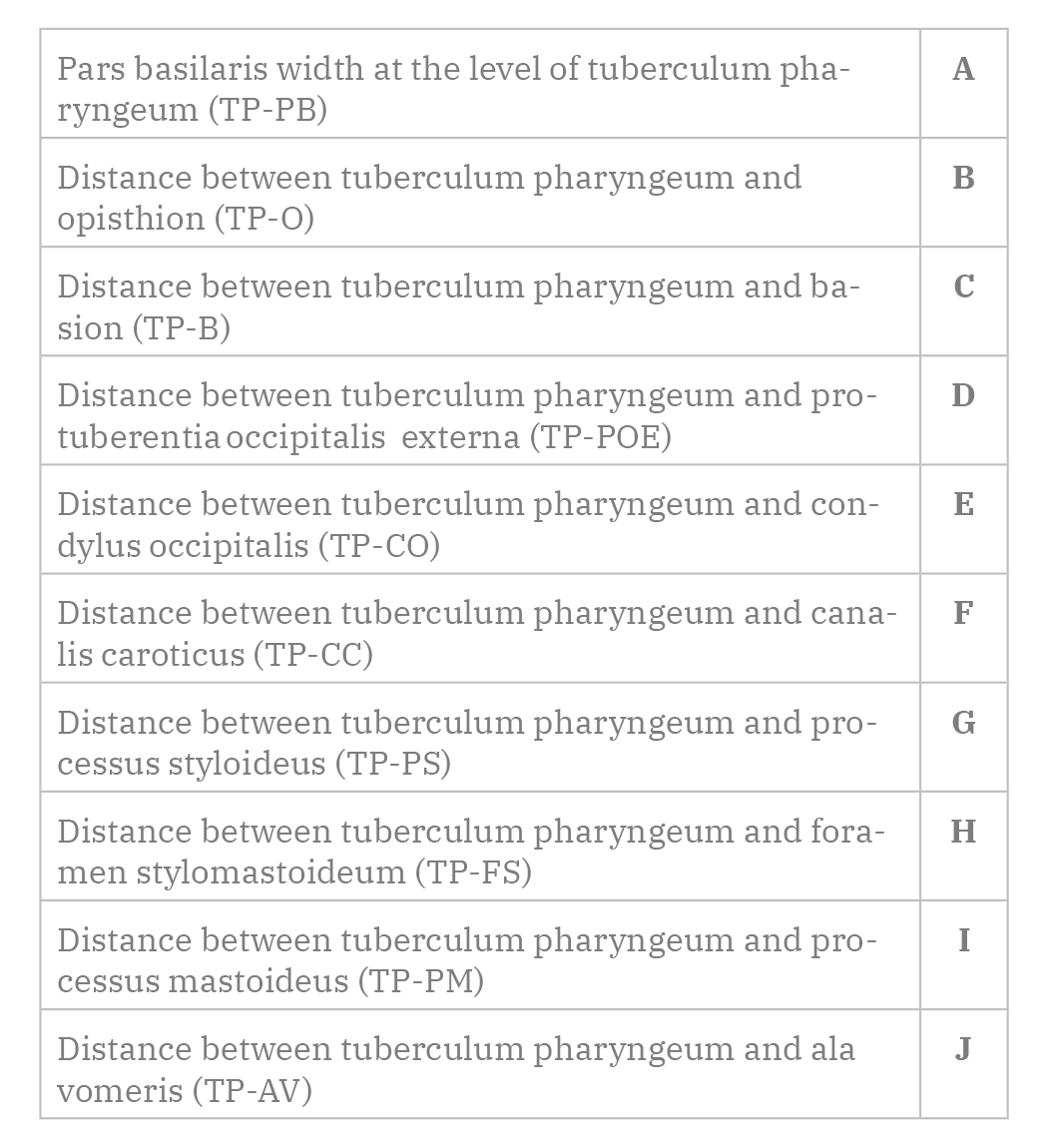 Table 1. The closest measurements between tuberculum pharyngeum and anatomic structures.
Table 1. The closest measurements between tuberculum pharyngeum and anatomic structures. Table 2. Descriptive statistics of quantitative variables in male and female groups (mm).
Table 2. Descriptive statistics of quantitative variables in male and female groups (mm).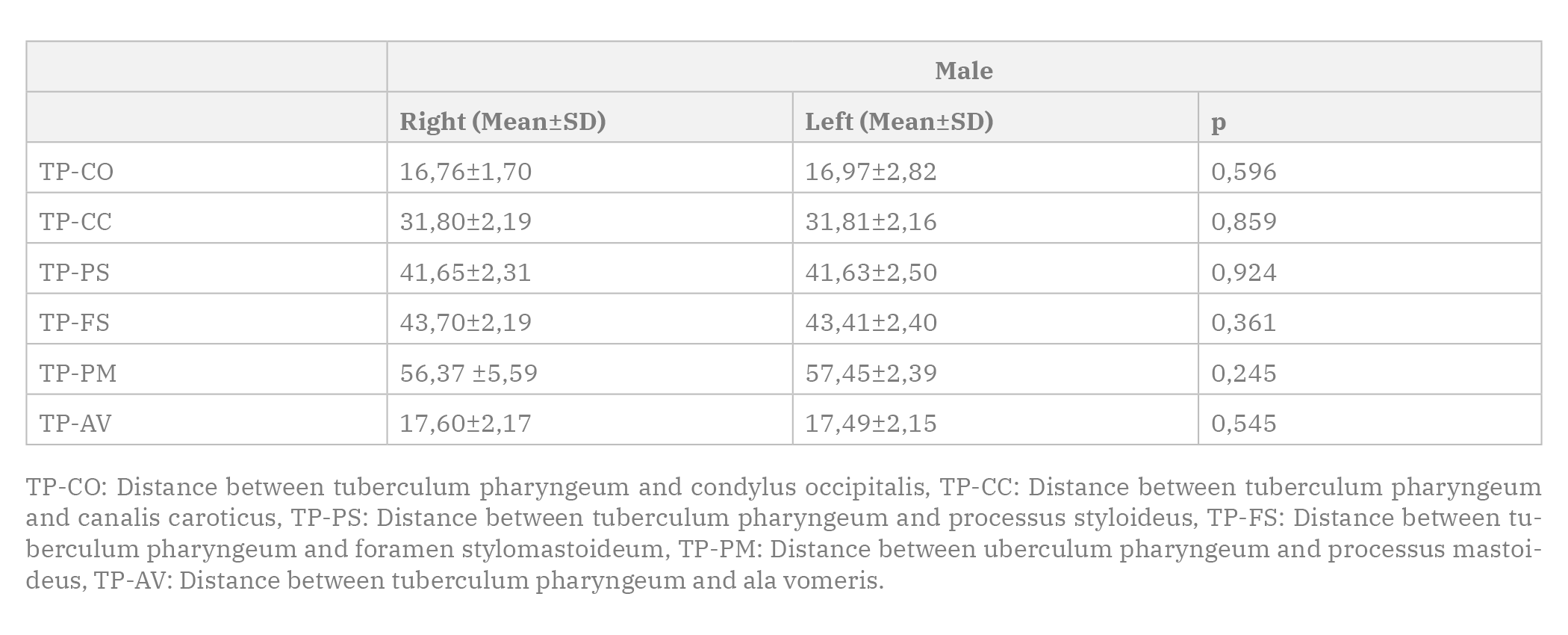 Table 3. Descriptive statistics of the dependent measurements in the male group (mm).
Table 3. Descriptive statistics of the dependent measurements in the male group (mm).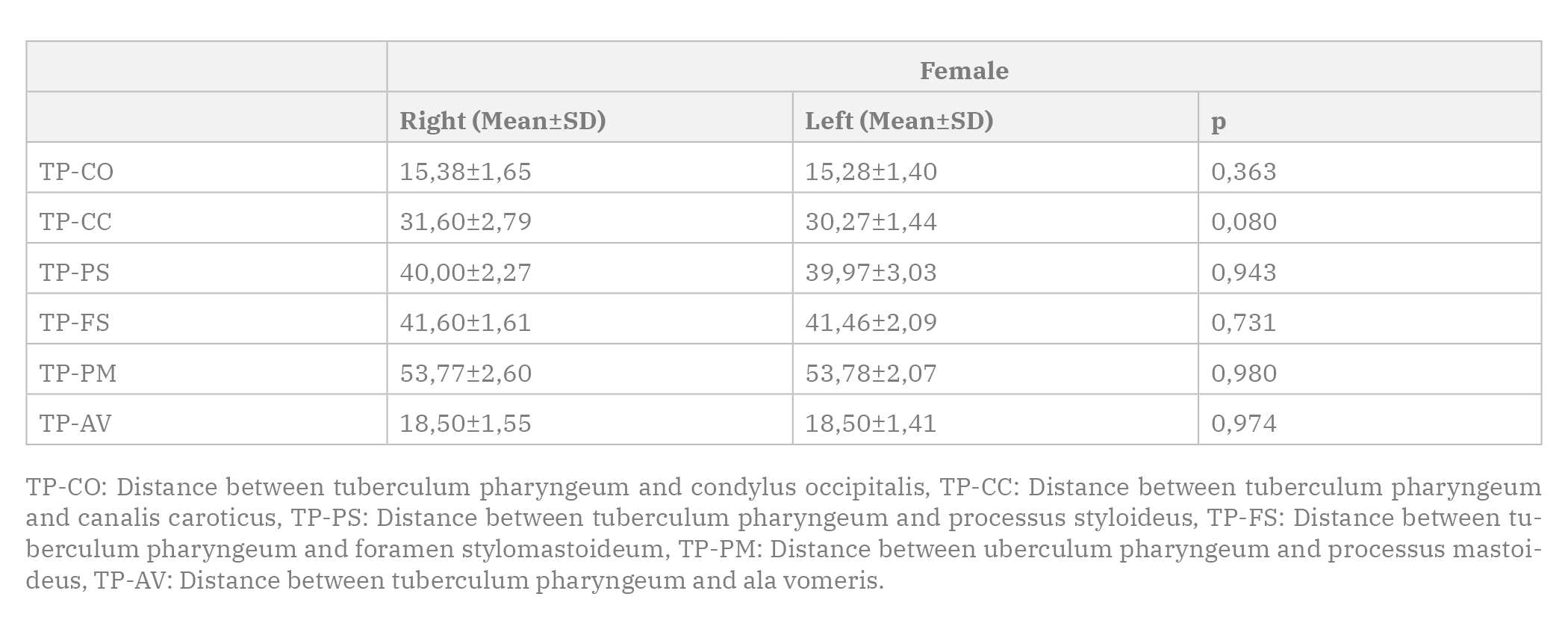 Table 4. Descriptive statistics of the dependent measurements in the female group (mm).
Table 4. Descriptive statistics of the dependent measurements in the female group (mm).AKTAS U, YILMAZLAR S, UGRAS N (2013) Anatomical restrictions in the transsphenoidal, transclival approach to the upper clival region: a cadaveric, anatomic study. J Cranio-Maxillofacial Surg, 41(6): 457-467.
AL-RUDAINY D, JU X, MEHENDALE FV, AYOUB A (2019) Longitudinal 3D assessment of facial asymmetry in unilateral cleft lip and palate. Cleft Palate-Craniofac J, 56(4): 495-501.
APARNA J, SANGEETHA S, PREMAVATHY D (2019) Anatomy and clinical significance of clivus and its neighboring structures. Drug Invention Today, 12(4): 774-776.
CANKAL F, UGUR HC, TEKDEMIR I, ELHAN A, KARAHAN T, SEVIM A (2004) Fossa navicularis: anatomic variation at the skull base. Clin Anat, 17(2): 118-122.
ERDEM H, KIZILKANAT ED, BOYAN N, SOAMES R, OGUZ O (2018) Anatomy and clinical importance of the extracranial clivus and surrounding structures. Int J Morphol, 36(2): 557-562.
HITOTSUMATSU T, MATSUSHIMA T, RHOTON JR AL (1999) Surgical anatomy of the midface and the midline skull base. Operative Techniques in Neurosurgery, 2(4): 160-180.
HOFMANN E, PRESCHER A (2012) The Clivus. Clin Neuroradiol, 22(2): 123-139.
JI W, WANG XY, XU HZ, YANG XD, CHI YL, YANG JS, YAN SF, ZHENG JW, CHEN ZX (2012) The anatomic study of clival screw fixation for the craniovertebral region. Eur Spine J, 21(8): 1483-1491.
KIZILKANAT ED, BOYAN N, SOAMES R, OGUZ O (2006) Morphometry of the hypoglossal canal, occipital condyle, and foramen magnum. Neurosurg Quart, 16(3): 121-125.
KRMPOTIĆ-NEMANIĆ J, VINTER I, EHRENFREUND T, MARUSIĆ A (2006) Age-related changes in the anatomical landmarks of the osseous epipharynx. Ann Anat, 188(5): 459-467.
LINDEN OE, HE JK, MORRISON CS, SULLIVAN SR, TAYLOR HO (2018) The relationship between age and facial asymmetry. Plastic Reconst Surg, 142(5): 1145-1152.
OZER MA, CELIK S, GOVSA F, ULUSOY MO (2011) Anatomical determination of a safe entry point for occipital condyle screw using three-dimensional landmarks. Eur Spine J, 20(9): 1510-1517.
PATEL CR, FERNANDEZ-MIRANDA JC, WANG WH, WANG EW (2016) Skull base anatomy. Otolaryngol Clin North Am, 49: 9-20.
SASAKI J, HASEGAWA S, YAMAMOTO S, WATANABE S, MIYACHI H, NAGAO T (2020) Relationship between facial asymmetry and positional plagiocephaly analyzed by three-dimensional computed tomography. J Cranio-Maxillofacial Surg, 48(3): 193-198.
SHARMA NA, GARUD RS (2011) Foramina of the posterior cranial base: a study of adult Indian skulls. Rev Arg Anat Clin, 3: 89-98.
STANDRING S (2016) Gray’s anatomy: the anatomical basis of clinical practice. 41th edition. Elsevier Health Sciences.
TAYLOR HO, MORRISON CS, LINDEN O, PHILLIPS B, CHANG J, BYRNE ME, FORREST CR (2014) Quantitative facial asymmetry: using three-dimensional photogrammetry to measure baseline facial surface symmetry. J Craniofac Surg, 25(1): 124-128.
WANG AJ, ZAIDI HA, LAWS JR ED (2016) History of endonasal skull base surgery. J Neurosurg Sci, 60(4): 441-453.
ZHONG S, REN J, ZHANG Y, LI W, LI H, SONG S, ZHAO G, CHENG Y (2018) Anatomic study of craniocervical junction and its surrounding structures in endoscopic transoral-transpharyngeal approach. J Craniofac Surg, 29(7): 1973-1977.