This study aimed to investigate the vertical symmetry of the external acoustic meatus (EAM) and its relationship with the occlusal plane in an Iranian population. The digital facial images of 220 individuals with a face-bow device were acquired. The image size was adjusted to the actual size, using a photo editing software. Also, the desired points and reference lines were measured and recorded by using the software tools. The collected data were analyzed, using Kolmogorov-Smirnov test, independent t-test, one-way ANOVA, and post-hoc test (α=0.05).
The higher position of the right ear EAM, the higher position of the left ear EAM, and their vertical symmetry were observed in 51.5%, 44.1%, and 4.5% of the images, respectively. The mean vertical distance between the meeting points of the right and left ear EAMs on the midsagittal plane, as well as the angle between the EAMs and the midsagittal plane, varied among three modes of the vertical symmetry of EAMs. However, no significant difference was found in the mean angle of the line crossing the EAM with the midsagittal line and the occlusal plane for the three modes. The results showed that the vertical symmetry of the EAMs was not correlated with sex or age. The vertical symmetry of the EAM was only observed in 4.5% of the participants.
Vertical symmetry of external auditory meatus and its relationship with the occlusal plane
Reza Soleimani1, Fahimeh Hamedirad2
1 Dental Faculty of Babol, University of Medical Sciences, Babol, Iran
2 Oral Health Research Center, Health Research Institute, Babol University of Medical Sciences, Babol, I.R. Iran
SUMMARY
Sign up or Login
INTRODUCTION
During dental treatments, the three-dimensional position of the maxillary and mandibular arches can be replicated in an articulator (Rosati et al., 2012; Chatuverdi and Thombare, 2013), using the face-bow transfer, which relates the maxillary cast to the articulator through the hinge axis relative to the reference points in the sagittal plane (e.g., the Frankfort horizontal plane or Camper’s plane) (Gandhi et al., 2017). Most patients have a degree of facial and craniofacial asymmetry, especially in the middle and lower thirds of the face (Porter and Olson, 2011). When a standard symmetric face-bow is used for a patient with an asymmetric external acoustic meatus (EAM), an error may occur in the transferred maxillary position relative to the sagittal axis. This makes the midline non-coincident with the midsagittal plane and raises the dental arch on one side; therefore, the occlusion may not be functional or esthetic (Shah et al., 2016; Wei et al., 2011; Gateno et al., 2003; Kim et al., 2010, 2014; Sherry and Jain, 2017; Naini, 2013).
On the other hand, standard measurements of the face are necessary to determine the occlusal plan. Variety in the position, size, and basic shape of the maxillofacial system has differences in the growth of these components in different populations, which in turn are influenced by certain genetic, climatic, and environmental factors. The results of anthropometric studies on the craniofacial characteristics of different racial groups have shown interregional diversity, and therefore the application of data from one ethnic group to another is misleading (Gandhi et al., 2017).
The present study was performed due to a lack of research on the symmetry of EAMs in an Iranian population and its importance in the success of dental treatments (Choi et al., 2015).
MATERIALS AND METHODS
This descriptive, analytical, cross-sectional study was conducted on 220 healthy adults during 2018-2019, using the available sampling method. The inclusion criteria were as follows: 1) age above 18 years; 2) willingness to participate in the study; 3) having a complete set of permanent teeth, excluding the third molars; 4) lack of dental crowns; 5) lack of orthodontic treatments; 6) no third molar extraction within the past six months; 7) no history of head and neck trauma or surgery or ear, nose, throat (ENT) surgery; 8) absence of craniofacial disorders, such as EAM abnormalities or apparent deformities in the maxilla and mandible; 9) known skin diseases with obvious effects on the appearance and soft facial tissue; and 10) lack of physical disabilities, restricting the face-bow application.
The participants entered the study after signing a written consent form. Some studies have used some techniques like MRI for determining the EAMs position (Tsutsumi et al., 2020). As these methods are unusual and expensive, we preferred to use simple clinical method that has been used in other studies (Hooda and D’Souza, 2012). To study the variables, two black bands were attached to the horizontal arm of the ear face-bow (Manico, Tehran, Iran) 10 cm apart and plotted to calibrate the size of digital images to the actual size. A black band was also attached to the ear rod arm for the ease of measurement. After the subject was seated, the ear face-bow was mounted without using a fork. A Fox plane (Manico, Tehran, Iran) was established tangentially to the maxillary occlusal plane and stabilized by occlusion with cotton rolls. It should be noted that the subject’s head did not bend to the right or left; both ears were clearly visible with no earrings; the trago-orbitale-tragion line was parallel to the floor; the lips were in rest; and the subject looked directly at the camera and raised his/her head until the philtrum was visible.
A digital camera (Canon 60D EOS, Ota, Tokyo, Japan), with a macro lens (Canon EF100mm f/2.8L IS USM Macro Lens, Ota, Tokyo, Japan) and a flash (Canon COOLPIX 270EX II; Canon Speedlite, Ota, Tokyo, Japan), was used to acquire images. To adjust the frame, the upper limit was tangential to the top of the participant’s head, and the lower limit was aligned in a way that the vertical and horizontal arms of the face-bow were completely inside the image; the focus point was placed directly on the eyes. The image was adjusted to the actual size in Photoshop CC 2019 (Adobe, USA), based on the ratio of actual size (a 10-cm band marked on the face-bow horizontal arm) to the digital format, as determined by the ruler tool in Photoshop. The reference points and the lines were determined by two independent observers, who were previously trained and synchronized regarding the methodology. Values were measured and recorded using the ruler tool.
Moreover, to examine the symmetry of the EAMs in Photoshop, the midpoint of the black bands on the outer edge of the right and left arms of the ear rods (the middle width of the ear rod arms) was defined as the midpoint of the EAM, from which the lines were drawn perpendicular to the midsagittal line. The alignment of these two lines indicated the vertical symmetry of the EAMs and the earholes. Next, using the Photoshop ruler tool (Fig. 1), the vertical distance between these lines in the midsagittal line, as well as the distance between the right and left EAMs on the midsagittal line, was measured. Afterward, the angle between the line of EAMs and the midsagittal line was measured. A line was also drawn parallel to the occlusal plane (based on the Fox plane) close to the line passing through the ears, and the angle was measured using the ruler tool. Moreover, the angle between the occlusal plane and the midsagittal line was measured and recorded (Fig. 2).
The collected data were analyzed in SPSS Version 20.0 (IBM, New York, USA), using Kolmogorov-Smirnov test, independent t-test, one-way ANOVA, and post-hoc test (α=.05).
RESULTS
A total of 220 individuals, aged 18 to 63 years, participated in this study. The reliability test, based on Cohen’s kappa coefficient, showed excellent agreement between the two examiners in evaluating different positions of vertical symmetry between the right and left EAMs (P<0.001; κ=0.898). Evaluation of the vertical symmetry of the right and left EAMs showed that 51.4% and 44.1% of the participants had the right and left EAMs in higher positions, respectively. Only in 4.5% of the participants, the two EAMs were vertically symmetric and aligned.
The mean vertical distance between the crossing lines of the right and left EAMs on the midsagittal line was 2.98±2.55 mm. The agreement between the two examiners in measuring other factors was excellent. The mean values measured by the two examiners were used to analyze facial dimensions. The mean distance between the ears and the midsagittal line is presented in Table 1. A significant difference was found in the mean vertical distance between the right and left EAM crossing points on the midsagittal line in different positions of the vertical symmetry of EAM (P=0.002).
The comparative analysis of the angles at different positions of the vertical symmetry of EAMs, based on one-way ANOVA, is shown in Table 2. A significant difference was found in the mean angle of the EAM lines with the midsagittal line in different positions of the vertical symmetry of EAM (P<0.001). The mean angles of the EAM lines with the midsagittal line and the occlusal plane were similar in different positions of the vertical symmetry of EAMs, and no significant difference was found (P=0.10 and P=0.766, respectively).
According to the present results, the mean distance of the right and left EAMs from the midsagittal line was significantly longer in males than females (P<0.001). However, no significant difference was found in terms of other factors. Also, there was no significant correlation between the vertical symmetry of EAM and sex (P=0.933; χ2=0.044). Similarly, changes in the measured factors were independent of age variations.
DISCUSSION
We did not find any studies on the vertical symmetry of EAM in an Iranian population. Only 4.5% of the participants had vertical symmetry in the right and left EAMs, and the majority had the right EAM in a higher position. Regarding the positional symmetry of the porion and EAM on the face and its correlation with maxillary occlusal plane rotation, the results showed that in both facial symmetry and asymmetry (including asymmetry with obvious maxillary occlusal rotation), the vertical porion tended to have a symmetric position. Since in facial asymmetry, the EAMs are positioned asymmetrically relative to the maxillary occlusal rotation, the possibility of EAM asymmetry must be considered for detecting and measuring maxillary rotation in facial asymmetry (Hooda and D’Souza, 2012). They found that in Indian population the left side is upper than the right side. The results of their study were the opposite of the results of our study.
Since the occlusal plane is adjusted in the patient’s mouth, according to the anatomical and esthetic criteria, when using a standard face-bow for transferring the rims to the articulator on a face with an asymmetric EAM, an error may occur in the transferred maxillary position relative to the sagittal axis. This makes the midline non-coincident with the midsagittal plane, raises the dental arch on one side, and therefore, results in a non-functional or non-esthetic occlusion (Shah et al., 2016; Wei et al., 2011; Gateno et al., 2003; Kim et al., 2010; Sherry and Jain, 2017; Naini, 2013). Moreover, the asymmetry of the external ear holes causes the rims to tilt in the articulator and causes confusion for the technician; also, occlusal errors may occur. As the higher position of one EAM than the other one (even 1 mm) results in a tilted upper jaw in the articulator, it is recommended to use a modified position of the ear rods to compensate for this asymmetry.
According to the present results, there was no significant difference in the mean distance of the right and left EAMs from the midsagittal line in different positions of the vertical symmetry of EAMs. In a study by Min-Gun Kim et al. on the 3D symmetry and alignment of skeletal porion and soft tissue, the anterior-posterior angular deviation between these two landmarks was measured. Their results showed that, in patients with facial asymmetry, the mean porion deviation was 3 mm, which should be considered during face-bow transfer (Choi et al., 2015). Moreover, in the present study, individuals with an apparent facial asymmetry were not studied, whereas the higher position of the right ear was observed in 51.4% of the participants. The vertical difference between the ears was 2.98±2.55 mm on average. However, one participant had a vertical difference of 15.3 mm, which required modification during the face-bow transfer.
In the present study, a significant difference was found in the mean vertical distance between the crossing points of the right and left EAMs on the midsagittal line in different positions of the EAM, and the mean distance in the symmetrical positions was less than the other two positions. This difference was attributed to the mean difference of distance in symmetric EAMs to either the higher right or left EAMs. When the EAMs are symmetric, the distance and the mean value will be zero for all individuals. Based on the statistical tests, the mean distance was 0.18 mm in the current study. The magnification error and the difference from the actual anatomic size seem to be associated with size measurements in Photoshop, depending on the software error for image analysis.
In a study by Mizgiryte et al. (2014), the mean angle between the EAM and the midsagittal plane was 90.12° (SD=1.48°) in the basal view and 90.36° (SD=2.25°) in the frontobasal view. In the current study, regardless of the mode of symmetry, the mean angle was 90.08° in the frontal view, which is consistent with the study by Mizgiryte and colleagues. Moreover, in the present study, the mean angle between the EAM lines and the occlusal plane, as well as the angle between the midsagittal line and the occlusal plane, were similar in different positions of the vertical symmetry of EAMs, and no significant difference was observed. This does not cause any problems in reconstructing the plane, except for cases where there is a significant difference. We suggest making a customized jig or using an approximate condylar axis or the pupillary line for face-bow recording. To the best of our knowledge, no similar research has been performed in this area; therefore, a comparison is not possible.
In the present study, the frequency distribution of the vertical symmetry of EAM was similar between men and women. The mean distance between the right and left EAMs and the midsagittal line was significantly longer in males than females, which could be attributed to the larger skeletal size of men than women. However, no significant difference was found in other linear and angular parameters in the two groups.
In a study by Djordjevic et al. (2014) on healthy Serbian adolescents, the total facial symmetry was lower in men than women (53.49% vs. 58.50%), although the difference was not clinically significant. In the present study, no significant difference was observed between male and female participants in terms of the vertical asymmetry of EAMs. In this regard, Sforza et al. compared the normal dimensions of the ears, the symmetry of the ears, and developmental changes from childhood to older age between male and female participants. Considering the significant sex-age interaction, the age pattern was different between men and women (Sforza et al., 2009). In the present study, no significant relationship was found with age, sex, or other variables. Given the high percentage of asymmetry in EAMs, design of a position modifier for the ear rods of the face-bow is recommended to compensate for this asymmetry.
Conclusion
According to the present results, the linear value of the mean vertical distance between the crossing points of the right and left ear EAMs on the midsagittal plane, as well as the angle between the EAM lines on the midsagittal plane, differed, depending on the vertical symmetry of the EAMs. However, no significant difference was found in the angle between the EAM lines and the occlusal plane in terms of symmetry. Also, changes in the linear and angular parameters were independent of age and sex.
Related articles


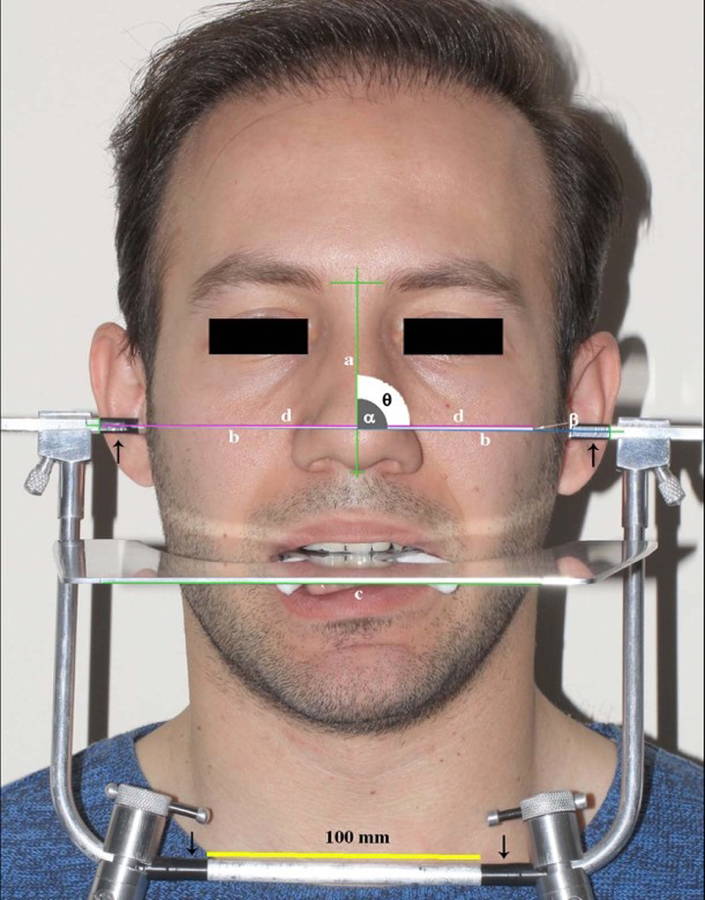 Fig. 1.- Matching of the images with software (Photoshop ruler tool).
Fig. 1.- Matching of the images with software (Photoshop ruler tool).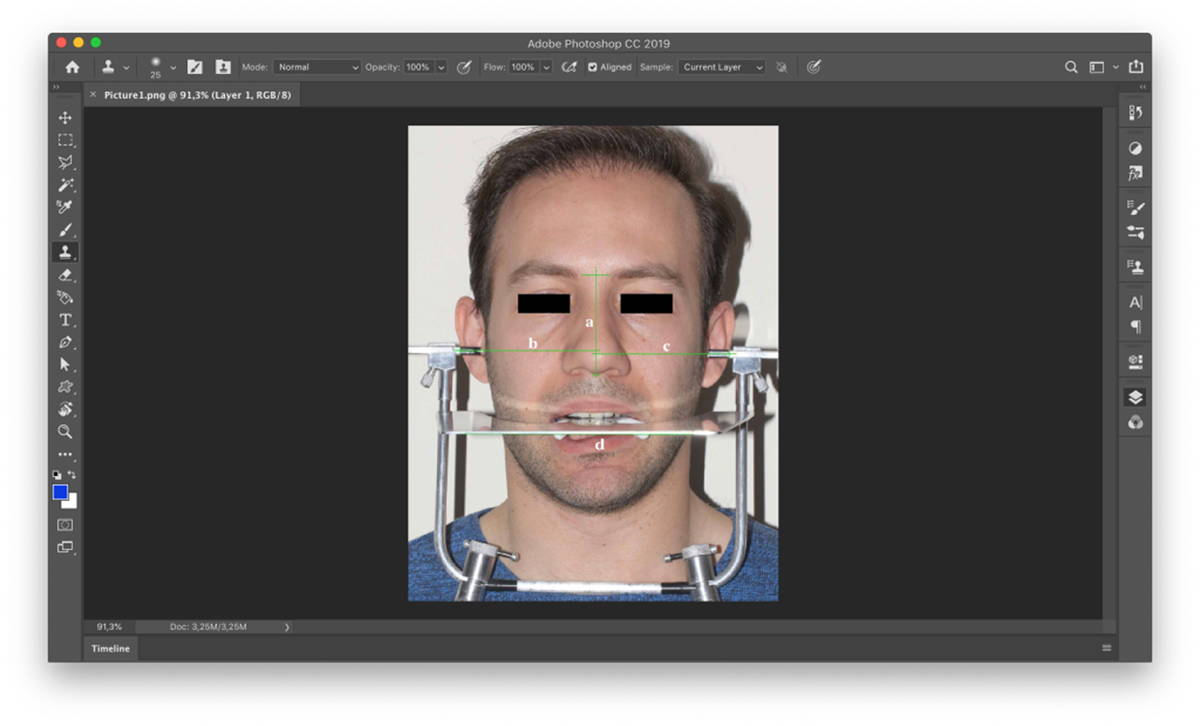 Fig. 2.- Placement of the Fox plane and the face-bow without fork on applicant’s face with black bands. The graphic lines and angles on the digital image including midsagittal line (a), the line between EAMs (b), the tangential line to the Fox plane (c), the parallel line to the Fox plane (d), the angle of the line between EAMs and midsagittal line (α), the angle of the line between EAMs and parallel line to the Fox plane (β), the angle between the midsagittal line and parallel line to the Fox plane (θ).
Fig. 2.- Placement of the Fox plane and the face-bow without fork on applicant’s face with black bands. The graphic lines and angles on the digital image including midsagittal line (a), the line between EAMs (b), the tangential line to the Fox plane (c), the parallel line to the Fox plane (d), the angle of the line between EAMs and midsagittal line (α), the angle of the line between EAMs and parallel line to the Fox plane (β), the angle between the midsagittal line and parallel line to the Fox plane (θ).CHATURVEDI S, THOMBARE R (2013) Cephalometrically assessing the validity of superior, middle and inferior tragus points on ala-tragus line while establishing the occlusal plane in edentulous patient. J Adv Prosthodont, 5: 58-66.
CHOI JW, JUNG SY, KIM HJ, LEE SH (2015) Positional symmetry of porion and external auditory meatus in facial asymmetry. Maxillofac Plast Reconstr Surg, 37: 33-37.
DJORDJEVIC J, TOMA AM, ZHUROV AI, RICHMOND S (2014) Three-dimensional quantification of facial symmetry in adolescents using laser surface scanning. Eur J Orthod, 36: 125-132.
GANDHI N, DANIEL S, KURIAN N (2017) Cephalometric study of the position of ala-tragus line in relation to Frankfort horizontal plane and occlusal plane among Ludhiana population. Indian J Dental Sci, 9: 165-169.
GATENO J, XIA J, TEICHGRAEBER JF, ROSEN A (2003) A new technique for the creation of a computerized composite skull model. J Oral Maxillofac Surg, 61: 222-227.
HOODA SH, D’SOUZA M (2012) Evaluation of facial asymmetry using digital photographs with computer aided analysis. J Indian Prosthodont Soc, 12: 8-15.
KIM BC, LEE CE, PARK W, KANG SH, ZHENGGUO P, YI CK, LEE SH (2010) Integration accuracy of digital dental models and 3-dimensional computerized tomography images by sequential point- and surface-based markerless registration. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 110: 370-378.
KIM MG, LEE JW, CHA KS, CHUNG DH, LEE SM (2014) Three-dimensional symmetry and parallelism of the skeletal and soft-tissue poria in patients with facial asymmetry. Korean J Orthodont, 44: 62-68.
MIZGIRYTE S, VAITELIS J, BARKUS A, ZALECKAS L, PLETKUS R, AUSKALNIS A (2014) Symmetry of external auditive meatus. A pilot study on human skulls. Stomatologija, 16: 102-108.
NAINI FB (2013) The Frankfort plane and head positioning in facial aesthetic analysis-the perpetuation of a myth. JAMA Facial Plast Surg, 15: 333-334.
PORTER JP, OLSON KL (2001) Anthropometric facial analysis of the African American woman. Arch Facial Plast Surg, 3: 191-197.
ROSATI R, ROSSETTI A, DE MENEZES M, FERRARIO VF, SFORZA C (2012) The occlusal plane in the facial context: inter-operator repeatability of a new three-dimensional method. Int J Oral Sci, 4: 34-37.
SFORZA C, GRANDI G, BINELLI M, TOMMASI DG, ROSATI R, FERRARIO VF (2009) Age-and sex-related changes in the normal human ear. Forensic Sci Int, 187: 1-7.
SHAH SZ, AZAD AA, HASSAN SH, ASLAM A (2016) Association of occlusal plane with the level of retromolar pad. Pakistan Oral Dental J, 36: 484-486.
SHERRY SA, JAIN AR (2017) Reliability of various craniofacial reference planes with occlusal plane in Dravidian population. J Pharm Res, 11: 1503-1505.
TSUTSUMI S, ONO H, ISHII H (2020) Positional relationship between the external acoustic meatus and sigmoid sinus: an MRI study. Surg Radiol Anat, 42: 791-795.
WEI R, CLAES P, WALTERS M, WHOLLEY C, CLEMENT JG (2011) Augmentation of linear facial anthropometrics through modern morphometrics: a facial convexity example. Aust Dent J, 56: 141-147.