The thumb is considered a marvelous piece of machinery, performing many versatile functions. The thumb is more prone for external injuries apart from the other pathologies which comprises about 5% of the emergencies treated. The external injuries can be treated by several reconstructive procedures such as tendon graft, tendon transfer etc., for which the abductor pollicis tendon can be used. Hence it is essential to know the morphometry and anatomical variations of abductor pollicis longus. 28 freshly embalmed human cadavers of both genders, which included 55 upper limbs, were dissected. The length, thickness, variation in the number and insertion of the abductor pollicis longus tendon were noted. The overall length of the abductor pollicis longus tendon was 63.62 ± 13.74 mm. The thickness of the tendon at the proximal, middle and at the distal level of insertion were 1.15 ± 0.56 mm, 1.02 ± 0.49 mm and 0.89 ± 0.48 mm respectively. No significant morphometric differences of length and thickness were observed between genders and between right and left side at distal level, whereas statistically significant difference exist at the proximal and middle level between the left and the right side. The results obtained from this study regarding the variations and morphometry of the abductor pollicis longus may be helpful for the surgeons in the various reconstructive procedures of the hand.
Morphometry of abductor pollicis longus relevant to surgical reconstruction of hand
Dhivyalakshmi Gnanasekaran, Raveendranath Veeramani, Aravindhan Karuppusamy, Grace Suganya
Department of Anatomy, Dhanvantri nagar, JIPMER, Puducherry, India 605006
SUMMARY
Sign up or Login
INTRODUCTION
The abductor pollicis longus (APL), is one of the extrinsic muscles of the thumb, which provides dynamic stability to it (Tsiouri et al., 2009; Biant, 2016; Hirschmann et al., 2014). Variation in the APL tendons has been implicated in the development of de Quervain’s tenosynovitis. Inadequate release of multiple tendons of APL in the extensor compartment of the wrist may result in the reoccurrence of de Quervain’s tenosynovitis (Kulthanan and Chareonwat, 2007). Variable insertion of the accessory slips of APL have been implicated in the development of thumb carpometacarpal joint arthritis or subluxation (Bravo et al., 2010; Schulz et al., 2002). But at the same time the additional slips have been used as grafting material for various tendon reconstruction surgeries (Bravo et al., 2010). Although the APL muscle and its variations have been studied since long, all these studies were done in western populations (Stein, 1951; Coleman et al., 1953; Jackson et al., 1986; Oudenaarde, 1991; Khoury et al., 1991; Brunelli and Brunelli, 1991; Godwin and Ellis, 1993; Bravo et al., 2010; El-Beshbishyet and Abdel-Hamid, 2013). Only a few studies have been carried out and there is paucity of knowledge regarding the variation of APL muscle, tendon and its dimension in the Indian literature (Joshi and Joshi, 2002; Tewari et al., 2015; Roy et al., 2012). The main objective of the present study is to find the incidence of variation in the APL muscle belly and the tendon, and also to document the detailed measurements of the APL tendon.
MATERIALS AND METHODS
The study was done in the department of anatomy, JIPMER, Puducherry from July 2016 to May 2018, after getting approval from the postgraduate research monitoring committee and the ethical clearance from the institute ethics committee. Twenty-eight formalin-fixed adult human cadavers of both genders available for undergraduate dissection in the Department of Anatomy, JIPMER, were taken up for the study. All embalmed cadavers without any damage were included in the study whereas, if there was any evidence of damage or loss of tissue in the region of the thumb, distal forearm and wrist were excluded. The right thumb of one of the female cadavers was amputated previously, hence a total sample of 55 upper limbs was included in the study.
The upper limb of the cadaver was kept abducted at the shoulder joint and in the supine position. The thumb was kept in extended position and the dissection was carried out. The distal forearm and hand were dissected in the dorsal aspect. The APL tendon inserted into the thumb was identified and traced backward. The course of the tendon and the muscle belly was traced by opening the first extensor retinaculum. Variations in the attachment of muscle, number of tendons and its site of insertion were noted. After dissection, the thumbs were photographed using a digital camera. Length of the tendon was measured from the distal end of the muscle fiber to the site of insertion of the tendon. The thickness of the tendon was measured at three places as follows: proximal— just after the ending of the muscle fibers at musculotendinous junction; middle—at the middle of the first dorsal compartment; and distal— just before its insertion. All the measurements were taken using mitutoyo digital Vernier caliper to the nearest millimeters (mm) by one single investigator. The results were expressed in range, mean, standard deviation and inter-quartile range. In case of multiple slips, the mean of the measurements of the multiple tendons were calculated for each hand and then compared between the left and right hands of matched pairs (27 hands). All relevant data were recorded and analyzed using IBM_PASW STATISTICS ver. 19.0 (SPSS ver 19.0). For left- and right-side comparison of the mean of the abovementioned quantitative variables, paired t-test (normal distribution) or Wilcoxon signed-rank test (non-normal distribution) were used. And for comparison between genders independent student t-test (normal distribution) and Mann Whitney U test (non-normal distribution) were used.
RESULTS
The APL muscle was present in all of the dissected hands (55 hands). The muscle was found to be fused with the extensor pollicis brevis (EPB) muscle to a variable degree from its origin until it gives rise to tendons in 54 hands. In one hand the EPB muscle belly and the tendon was absent, so an independent APL muscle belly was seen in this case (Fig. 1d). But in other 54 hands, an identifiable fascial plane separating both the APL and EPB muscle was found at least in the distal end of the muscle fiber. Hence no separate or distinct APL muscle belly was seen in 98% (54 hands). There was also no additional APL muscle belly.
Single APL tendon was not observed in any of the dissected hands. The number of APL tendons observed ranges from two to six (Fig. 1). The frequency distribution of number of APL tendon in each hand is given in Fig. 2.
The APL tendon inserts into the base of the first metacarpal in the majority of hands. Some of the tendons also get inserted into the thenar muscle (Fig. 3a), into the trapezium (Fig. 3b), part of tendon into the trapezium and partly into the thenar muscle (Fig. 3.c), and sometimes it also gets inserted partly into the base of the first metacarpal and the remaining into the thenar muscle (Fig. 3d). In one hand where the EPB muscle and the tendon was absent, it was found that one of the five tendons of the APL muscle inserted into the base of the proximal phalanx instead of the normal EPB tendon (Fig. 1d). The frequency distribution of APL tendon based on the site of insertion is given in Fig. 4.
More than one APL tendon was present in 100% of the dissected hands (55 hands). Hence in total 186 tendons, measurements were taken up for the analysis. The overall length and thickness of the APL tendon is provided in Table 1. The average of the measurements such as length of the APL tendons and thickness of the tendons at proximal, middle and distal level showed no significant difference between male and female (Table 2).
The mean length of the APL tendon measured in the left side (94 tendons) and right side (92 tendons) was 65.22 mm and 61.50 mm. The thickness of the tendons measured at the proximal, middle and distal level on the left side were 1.23 mm, 1.08 mm, 0.91 mm and the same measured on the right side were 1.06 mm, 0.95 mm and 0.86 mm respectively.
The average of the measurements related to the APL tendons were compared between the matched pairs (27 hands). No significant differences were observed between the left and the right side related to the measurements such as length of the tendon and the thickness at distal level. But there exists significant difference in the thickness of the tendon at proximal and at middle level between the left and the right side (Table 3).
DISCUSSION
The present study involved dissection of 55 upper limbs to study the APL muscle. Out of these 55 limbs, the independent APL muscle was seen in only one of the dissected hands whereas the muscle was found to be fused with extensor pollicis brevis muscle to a variable extent in the remaining 54 hands. Fabrizio and Clemente (1996) observed variation in the APL muscle belly in 30% (15 out of 50 hands) of dissected hands. In all of these hands, an additional APL muscle belly was found to arise from the lateral aspect of distal portion of normal APL muscle (Fabrizio and Clemente, 1996). In another study, two independent APL muscle bellies were found in 20% (16 out of 78 hands) (Bravo et al., 2010). Rarely, the APL having three independent muscle bellies have also been documented in the literature (Sarikcioglu and Abdel-Hamid, 2004). While in the other study, the APL muscle was identified with two muscle bellies with each one giving rise to an independent tendon. Of these two tendons, one tendon was inserted into the first metacarpal and the other tendon again split into three to insert into the abductor pollicis brevis, opponens pollicis, and flexor pollicis brevis muscles. The tendon slip inserted into the abductor pollicis brevis was described to have acquired muscular characteristics before insertion (Yuksel et al., 1992). Brandsma et al. (1996) suggested that such insertion of the APL into the abductor pollicis brevis can be considered a digastric muscle (one long muscle with two bellies).
In our study, single APL tendon was not seen in any of the dissected hands, similar to El-Beshbishy and Abdel-Hamid (2013). Two tendons were observed in 31%. Three tendons and four tendons were observed in 25% each. In 11% five tendons were observed and six tendons in 7% of the dissected hands. Variations in the number of the APL tendons were reported to be ranging from one to six in numbers. Some studies have even reported up from seven to nine APL tendon slips (Sarikcioglu and Yildirim, 2004; Mansur et al., 2010). The incidence of the number of APL tendon slips in various studies is given in Table 4. Melling et al. (1996) stated that multiple slips of APL are also observed in other primates like gorillas and gibbons, suggesting the possibility of APL being an atavistic structure in humans.
Regarding the insertion of APL tendon, it was observed from this study that APL tendons inserted most commonly into the base of the first metacarpal bone (66%), similar to other studies. And insertion of the tendons into the trapezium was seen in only 19% in the present study, which is similar to the study by Roy et al. (2012). Tewari et al. (2015) reported such type of insertion was seen in 41% and on the other hand Khoury et al. (1991) could see it in 6% only. Brunelli and Brunelli (1992) opined from their cadaveric study that absence of insertion of the tendon into the trapezium should be regarded as normal as it was seen in 71% cases. It was claimed that absence of insertion into the trapezium could result in instability and arthritis of the trapeziometacarpal joint (Brunelli and Brunelli, 1992). Abnormal insertion of all four slips of APL into the fascia of APB muscle has resulted in laxity and recurrent subluxation of the trapeziometacarpal joint (Martinez and Omer, 1985). In the present study no insertion of the tendons into the thenar fascia was seen. Apart from insertion of the APL muscle into the base of first metacarpal, variable insertion site of these accessory tendons has been reported in the literature. Additional insertion sites of the APL tendon documented in the literature were the trapezium bone, the opponens pollicis or the abductor pollicis brevis muscle. Few cases have reported about insertion into the flexor pollicis brevis muscle, the scaphoid bone, fascia covering the thenar muscle, capsule of the trapeziometacarpal joint, anterior oblique ligament of this joint capsule and thumb proximal phalanx’ base. Rarely, it was documented to insert into the wrist extensor retinaculum (Sarikcioglu and Yildirim, 2004, Kocabiyik et al., 2009). The tendons of the APL were considered to stabilize the carpometacarpal joint of the thumb (Fabrizio and Clemente, 1996). Sometimes the distal extension of APL muscle belly into the first extensor compartment produces painful thumb and wrist on movement (Patel et al., 1988). In our study no such extension of APL muscle belly into the extensor compartment was observed. The variations in the site of insertion of the APL tendon in various studies are given in Table 5.
The embryological reasons of multiple slips and its variable distal attachments could be due to persistence of an early embryonic developmental state of APL muscle. In a human embryo with a crown-rump length of 20 mm the differentiating APL tendon is divided into three strips; the palmar slip blended with the opponens pollicis, middle inserts into the trapezium and the dorsal into the base first metacarpal. Later, when the crown-rump length becomes 60 mm various new connections are established between the palmar strip and adjacent abductor pollicis brevis meanwhile the connection with the opponens pollicis is lost. This supports our study as more than one APL tendons was observed in all the 55 hands (Tewari et al., 2015).
Only very few studies have measured the dimensions of the APL tendons and they followed different methodology. There was difference in the grouping of the APL tendon slips. El-Beshbishy and Abdel-Hamid (2013) classified the tendon slips into two groups. Those tendons that were lying adjacent to the EPB muscle were regarded as normal APL tendons (lateral group), while other tendons lying medially were regarded as the accessory tendons (medial group) (El-Beshbishy and Abdel-Hamid, 2013). Bravo et al. (2010) considered that the tendon slips radial to the main APL tendon and lying close to the EPB as the accessory ones. Bravo et al. (2010) measured the thickness and width of the main and accessory tendons at its insertion site. We could not compare our study results related to the tendons dimension with that of Bravo et al. (2010) and of El-Beshbishy and Abdel-Hamid (2013). Melling et al. (1996) suggested that the number, thickness and length of the accessory tendons of APL and EPB might have an important function in the development of de Quervain’s disease.
Therefore, the knowledge of anatomical variations, arrangements, and prevalence of the multiple tendons of APL is of utmost importance for the physicians and surgeons to diagnose and treat various clinical conditions arising out of it, for repairing the injured tendons and during reconstructive surgery involving tendon transfer, tendon graft etc.
Related articles


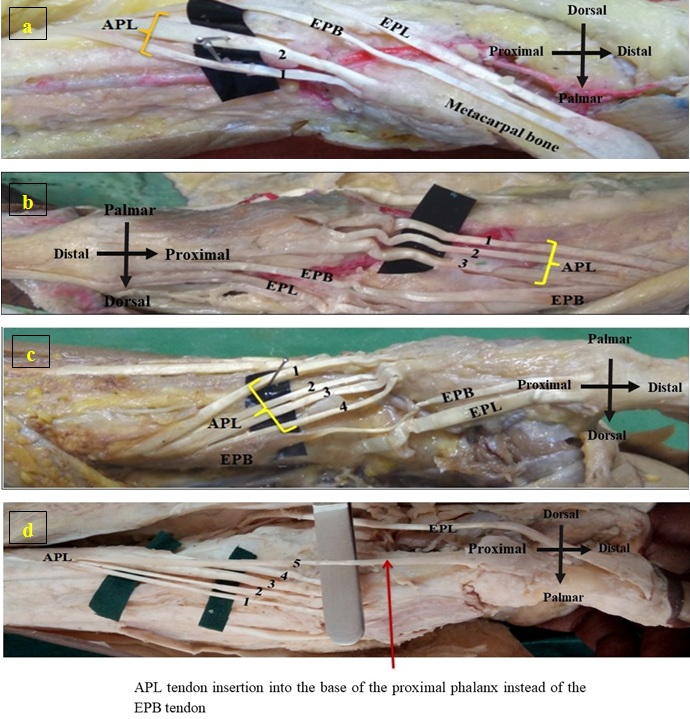 Fig. 1.- Variation in the number of APL tendons. a. Two, b. Three, c. Four, d. Five APL tendons. In figure d 5 independent APL muscle belly with absent EPB muscle belly and APL tendon number 5 attached to the base of the proximal phalanx instead of EPB tendon. APL - Abductor Pollicis Longus; EPB - Extensor Pollicis Brevis.
Fig. 1.- Variation in the number of APL tendons. a. Two, b. Three, c. Four, d. Five APL tendons. In figure d 5 independent APL muscle belly with absent EPB muscle belly and APL tendon number 5 attached to the base of the proximal phalanx instead of EPB tendon. APL - Abductor Pollicis Longus; EPB - Extensor Pollicis Brevis.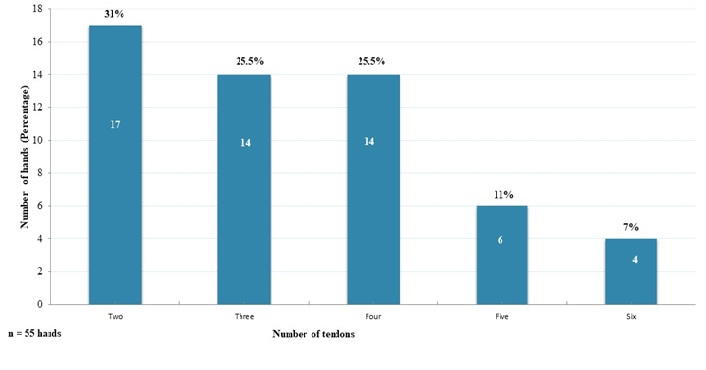 Fig. 2.- Distribution of number of abductor pollicis longus tendon per hand.
Fig. 2.- Distribution of number of abductor pollicis longus tendon per hand.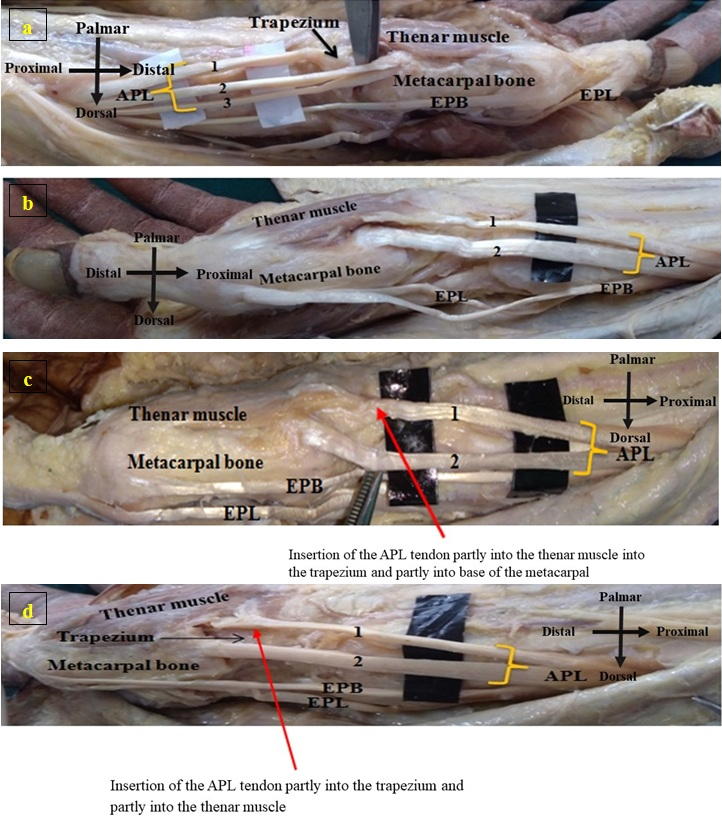 Fig. 3.- Variation in the insertion of APL tendons. a. Insertion of tendon 1 into thenar muscle. b. Insertion of tendon 1 into the trapezium. c. Insertion of tendon 1 partly into the thenar muscle and partly into the trapezium. d. Insertion of tendon 1 partly into the thenar muscle and partly into the metacarpal. APL - Abductor Pollicis Longus; EPB - Extensor Pollicis Brevis; EPL - Extensor Pollicis Longus.
Fig. 3.- Variation in the insertion of APL tendons. a. Insertion of tendon 1 into thenar muscle. b. Insertion of tendon 1 into the trapezium. c. Insertion of tendon 1 partly into the thenar muscle and partly into the trapezium. d. Insertion of tendon 1 partly into the thenar muscle and partly into the metacarpal. APL - Abductor Pollicis Longus; EPB - Extensor Pollicis Brevis; EPL - Extensor Pollicis Longus.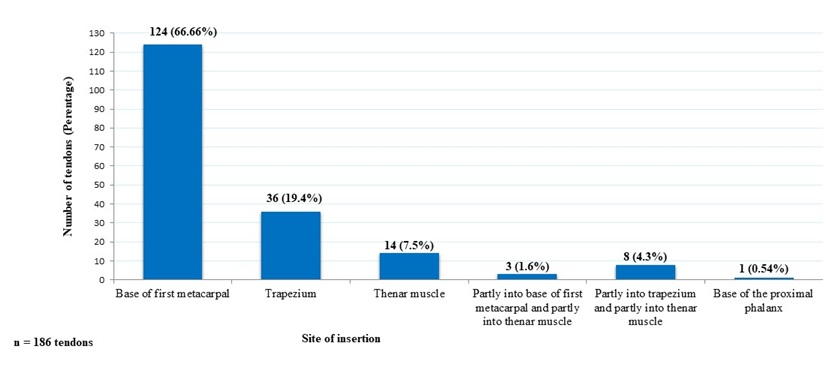 Fig. 4.- Distribution of abductor pollicis longus tendon based on the site of insertion.
Fig. 4.- Distribution of abductor pollicis longus tendon based on the site of insertion.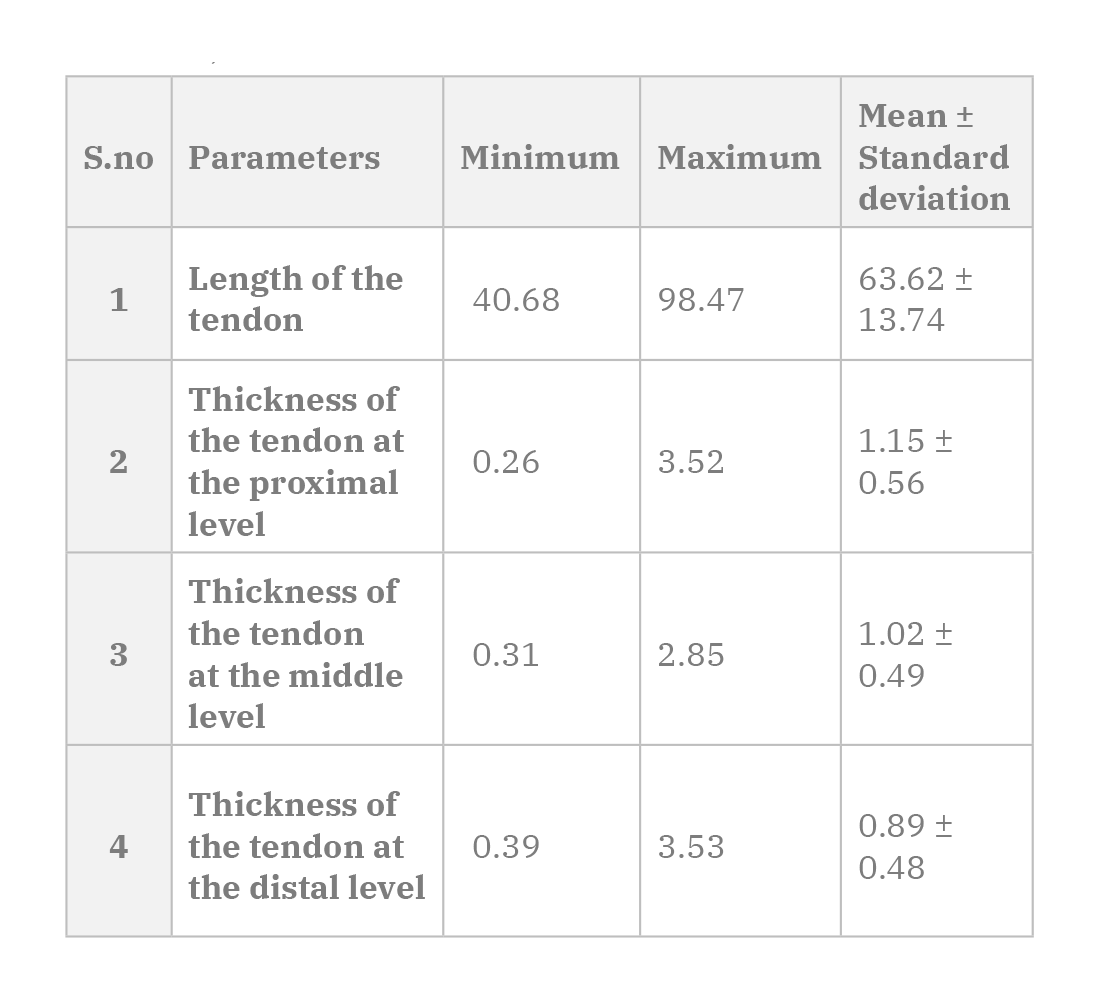 Table 1. Overall length and thickness of the abductor pollicis longus tendon (mm); (Minimum, maximum, mean ± standard deviation) n=186 tendons.
Table 1. Overall length and thickness of the abductor pollicis longus tendon (mm); (Minimum, maximum, mean ± standard deviation) n=186 tendons.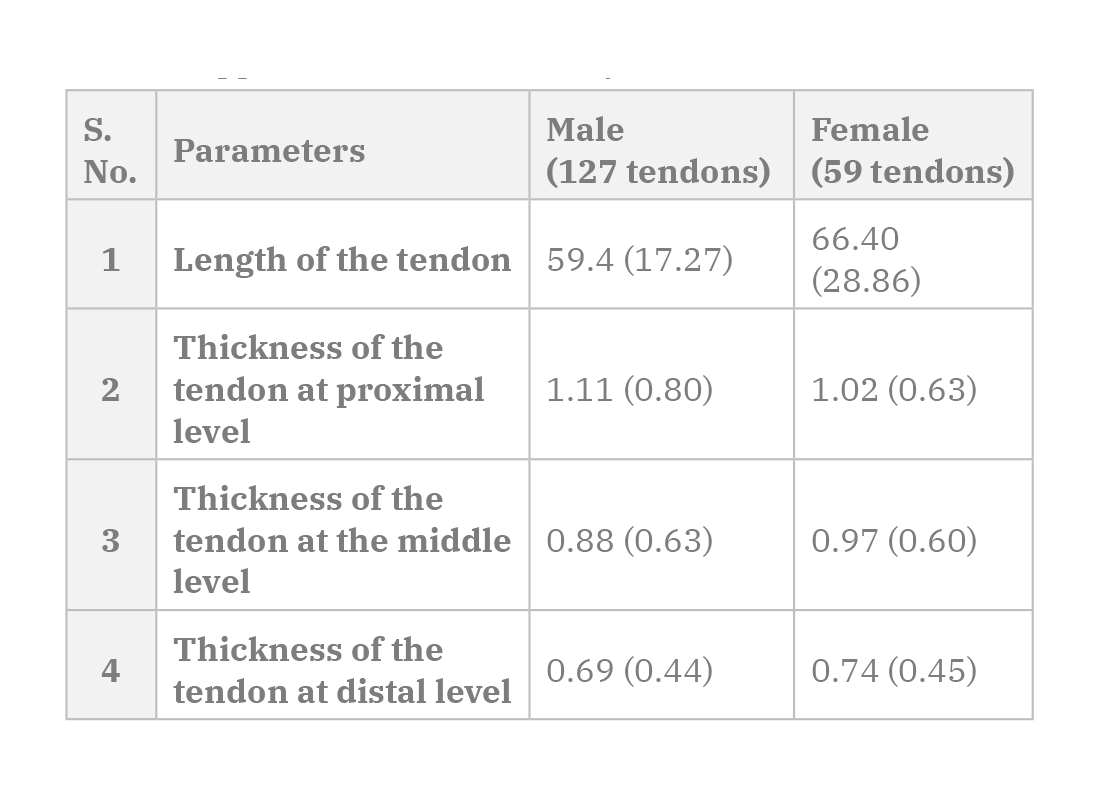 Table 2. Comparison of length and thickness of the abductor pollicis longus tendons between the genders (mm); Median (Interquartile range); n = 186 tendons; All the parameters measured showed non-normal distribution. Mann-Whitney U test was applied for statistical analysis.
Table 2. Comparison of length and thickness of the abductor pollicis longus tendons between the genders (mm); Median (Interquartile range); n = 186 tendons; All the parameters measured showed non-normal distribution. Mann-Whitney U test was applied for statistical analysis.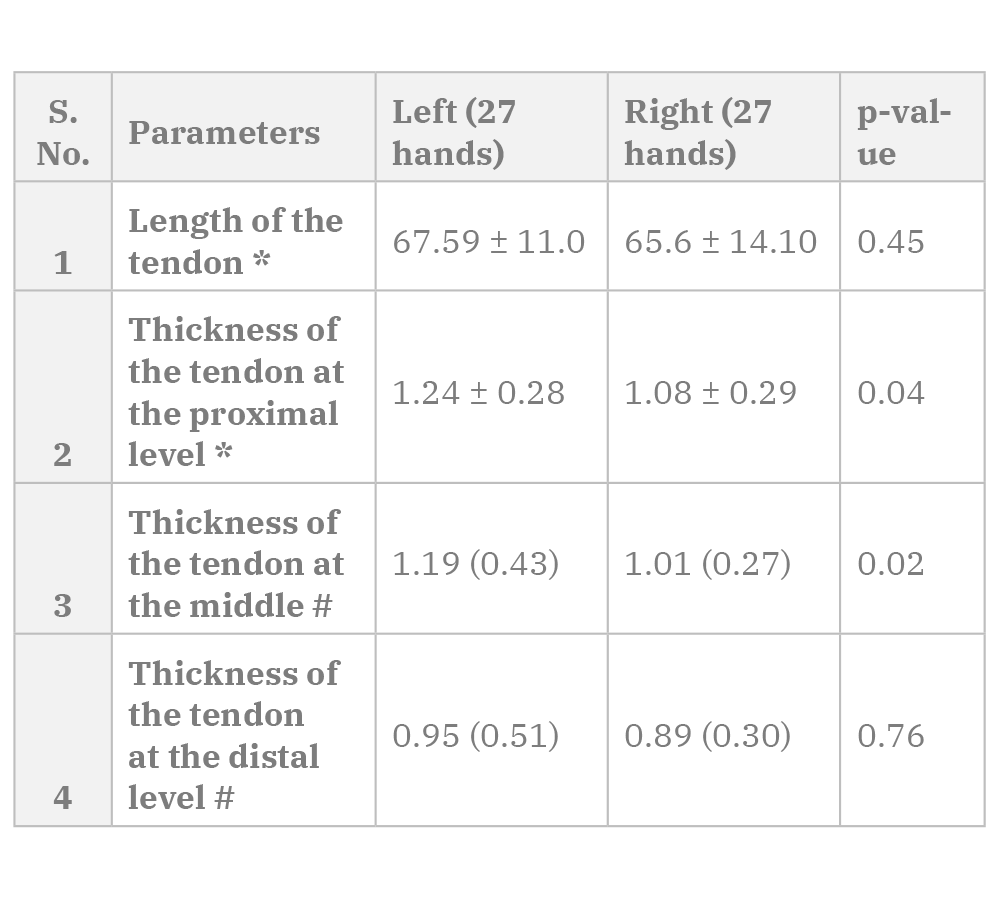 Table 3. Comparison of mean length and thickness of the abductor pollicis longus tendon between paired limbs (mm); [Mean ± Standard deviation/ Median (Interquartile range)]. * paired sample t-test; # Wilcoxon signed-rank test was applied for statistical analysis.
Table 3. Comparison of mean length and thickness of the abductor pollicis longus tendon between paired limbs (mm); [Mean ± Standard deviation/ Median (Interquartile range)]. * paired sample t-test; # Wilcoxon signed-rank test was applied for statistical analysis.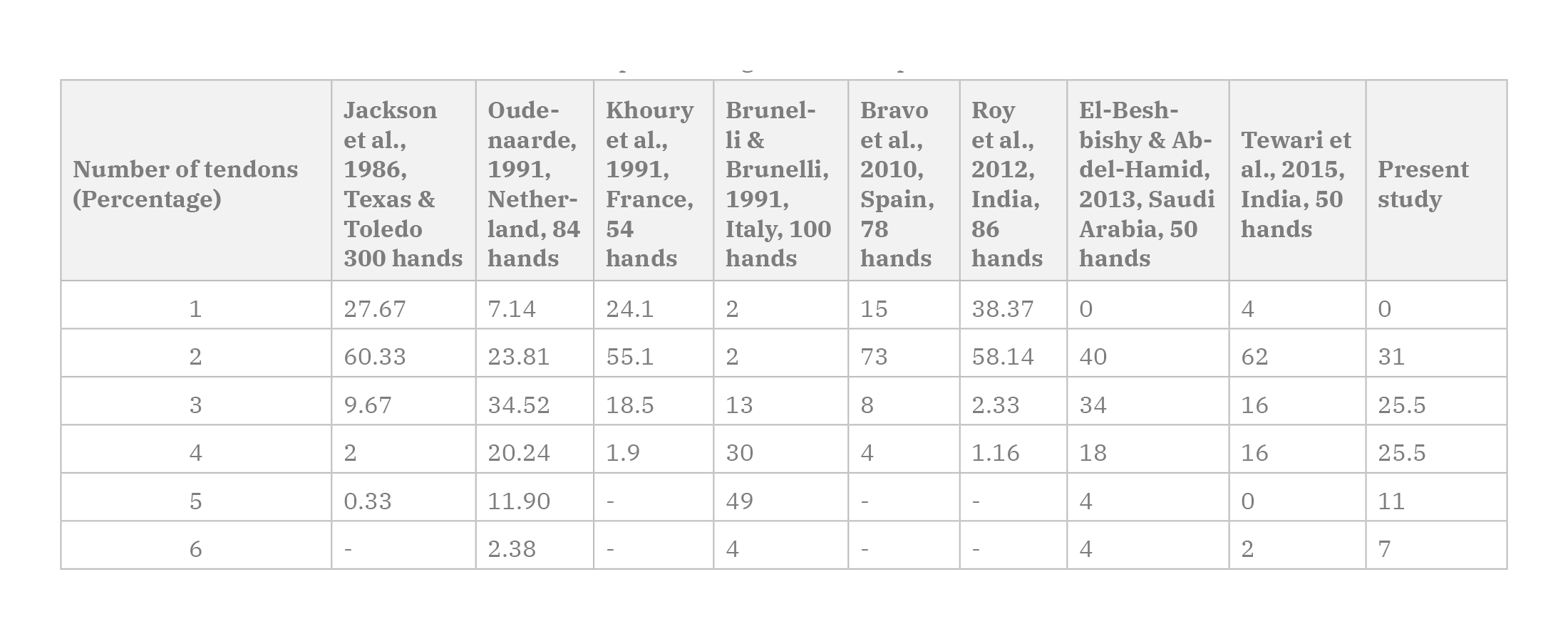 Table 4. The incidence of the number of abductor pollicis longus tendon slips in various studies.
Table 4. The incidence of the number of abductor pollicis longus tendon slips in various studies.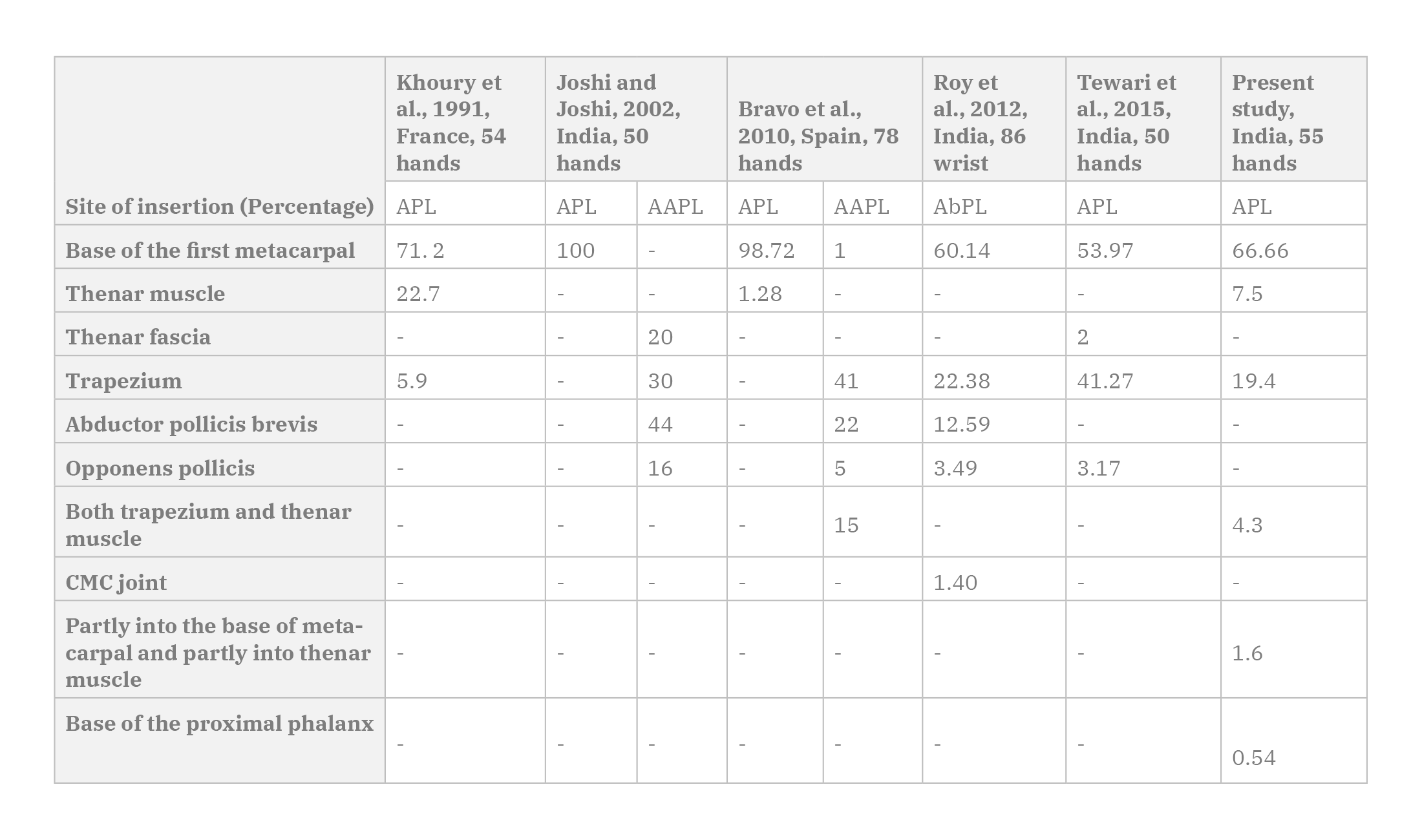 Table 5. Comparison of variation in the site of insertion of abductor pollicis longus tendon with other studies. APL - Abductor Pollicis Longus; AAPL - Accessory Abductor Pollicis Longus.
Table 5. Comparison of variation in the site of insertion of abductor pollicis longus tendon with other studies. APL - Abductor Pollicis Longus; AAPL - Accessory Abductor Pollicis Longus.BIANT LC (2016) Elbow and forearm. In: Standring S (ed). Gray’s Anatomy: the anatomical basis of clinical practice. 41st ed. New York: Elsevier Limited, pp 837-861.
BRANDSMA JW, OUDENAARDE EV, OOSTENDROP R (1996) The abductores pollicis muscles: clinical considerations based on electromyographical and anatomical studies. J Hand Ther, 9(3): 218-222.
BRAVO E, BARCO R, BULLON A (2010) Anatomic study of the abductor pollicis longus: a source for grafting material of the hand. Clin Orthop Relat Res, 468(5): 1305-1309.
BRUNELLIG A, BRUNELLI GR (1992) Anatomy of the extensor pollicis brevis muscle. J Hand Surg, 17(3): 267-269.
COLEMAN SS, McAFEE DK, ANSON BJ (1953) The insertion of the abductor pollicis longus muscle. an anatomical study of 175 specimens. Quart Bull Northwestern Univ Med School, 27(2): 117-122.
EL-BESHBISHY RA, ABDEL-HAMID GA (2013) Variations of the abductor pollicis longus tendon: an anatomic study. Folia Morphol (Warsz), 72(2): 161-166.
FABRIZIO PA, CLEMENTE FR (1996) A variation in the organization of abductor pollicis longus. Clin Anat, 9(6): 371-375.
GODWIN Y, ELLIS H (1993) Anatomical study of the symmetry of lateral extensor compartment of the wrist. Clin Anat, 6(4): 222-225.
HIRSCHMANN A, SUTTER R, SCHWEIZER A, PFIRRMANN CW (2014) MRI of the thumb: anatomy and spectrum of findings in asymptomatic volunteers. Am J Roentgenol, 202(4): 819-827.
JACKSON WT, VIEGAS SF, COON TM, STIMPSON KD, FROGAMENI AD, SIMPSON JM (1986) Anatomical variations in the first extensor compartment of the wrist. J Bone Joint Surg Am, 68(6): 923-926.
JOSHI SS, JOSHI SD (2002) Applied significance of variations of the first extensor compartment of wrist. J Anat Soc India, 51(2): 159-161.
KHOURY Z, BERTELLI J, GILBERT A (1991) The subtendons of the abductor pollicis longus muscle. Surg Radiol Anat, 13(3): 245-246.
KOCABIYIK N, TATAR I, YALCIN B, YAZAR F, OZAN H (2009) Tendon variations of extensor digitorum and abductor pollicis longus muscles. IJAV, 2: 54-56.
KULTHANAN T, CHAREONWAT B (2007) Variations in abductor pollicis longus and extensor pollicis brevis tendons in the Quervain syndrome: a surgical and anatomical study. Scand J Plast Reconstr Surg Hand Surg, 41(1): 36-38.
MANSUR DI, KRISHNAMURTHY A, NAYAK SR, KUMAR CG, RAI R, D’COSTA S, PRABHU LV (2010) Multiple tendons of abductor pollicis longus. IJAV, 3: 25-26.
MARTINEZ R, OMER JR (1985) Bilateral subluxation of the base of the thumb secondary to an unusual abductor pollicis longus insertion: a case report. J Hand Surg Am, 10(3): 396-399.
MELLING M, WILDE J, SCHNALLINGER M, SCHWEIGHART W, PANHOLZER M (1996) Supernumerary tendons of the abductor pollicis. Acta Anat, 155(4): 291-294.
MILETIN J, SUKOP A, BACA V, KACHLIK D (2017) Arterial supply of the thumb: systemic review. Clin Anat, 30(7): 963-973.
PATEL MR, DESAI SS (1988) Anomalous muscles of the first dorsal compartment of the wrist. J Hand Surg Am, 13(6): 829-831.
ROY AJ, ROY AN, DE C, BANERJID, DAS S, CHATTERJEE B, HALDER TC (2012) A cadaveric study of the first dorsal compartment of the wrist and its content tendons: anatomical variations in the Indian population. J Hand Microsurg, 4(2): 55-59.
SARIKCIOGLU L, YILDIRIM FB (2004) Bilateral abductor pollicis longus muscle variation: Case report and review of the literature. Morphologie, 88(282): 160-163.
SCHULZ CU, ANETZBERGER H, PFAHLER M, MAIER M, REFIOR HJ (2002) The relation between primary osteoarthritis of the trapeziometacarpal joint and supernumerary slips of the abductor pollicis longus tendon. J Hand Surg Br, 27(3): 238-241.
STEIN AD (1951) Variations of the tendons and insertions of the abductos pollicis longus and extensor pollicis brevis. Anat Rec, 110(1): 49-55.
TEWARI J, MISHRA PR, TRIPATHY SK (2015) Anatomical variation of abductor pollicis longus in Indian population: A cadaveric study. Indian J Orthop, 49: 549-553.
TSIOURI C, HAYTON MJ, BARATZ M (2009) Injury to the ulnar collateral ligament of the thumb. Hand (NY), 4(1): 12-18.
VAN OUDENAARDE E (1991) Structure and function of the abductor pollicis longus muscle. J Anat, 174: 221.
YUKSEL M, ONDERAGLU S, ARIK Z (1992) Case of an abductor pollicis longus muscle: variation or differentiation? Okajimas Folia Anat Jpn, 69(4): 169-171.