Earlier studies on growth and estimation of age from fetal bones were analyzed from photographs, radiographs, ultrasonographs and bones from chemically preserved fetuses. The earlier findings might not be applicable when information about growth and age estimation are sought from the naturally macerated fetal bones. The present study was undertaken in the Department of Anatomy, BJ Medical College, Pune, India with the aim to study the growth of fetal radius and also to estimate the CRL (crown-rump length) and CHL (crown-heel length) of fetuses based on osteometry on fetal radius. A natural process of maceration technique was adopted to prepare the bones. Osteometry was taken directly on fetal radius. CRL and CHL were taken from fresh fetuses. There were seven osteometric measurements (five measurements were newly introduced) taken on 912 fetal radii (right and left) from 456 fetuses (244 males and 212 females) from Indian population. The fetuses had the age range between 11 weeks to 40 weeks of intrauterine life. It was observed that 8.04% showed significant side differences and 12.5% showed significant sex differences based on the osteometry. There was positive growth trend found in fetal radius on the basis all the osteometric measurements. The Maximum Length of Radius (r-ml) showed the fastest rate of growth in females during weeks 11 to 16 of intrauterine life. For every 1 mm in the CRL, the r-ml was increased by .235 mm. Regression equations were calculated to estimate the CRL and CHL from the osteometry done on fetal radius. Growth study of the fetal radius has its anatomical significance. Age estimation is a crucial factor in dealing with forensic and archaeological anthropology.
Growth of radius and estimation of crown-rump length and crown-heel length based on osteometry on the diaphysis of human fetal radius
Dhason Simon1, Don Varghese2, Annie Varghese3, Biswajit Bhowmick4, Monie Simon5
1 College of Health Sciences, Arsi University, Asella, Ethiopia
2 Specialist Oral and Maxillofacial Surgeon, Saudi German Hospital, Dubai, UA
3 IBN SINA Medical Centre, Dubai, UAE
4 Senior Medical Officer, Army Medical Core, India
5 Chellaram Hospital (Diabetes Care & Multispeciality), Pune - 411021, India
SUMMARY
Sign up or Login
INTRODUCTION
Somatometric and osteometric studies on the human fetus help understand the anatomical growth pattern and development of the human fetus. This paper presents a study on fetal skeletal growth of the radius based on a new fetal skeletal collection obtained by natural maceration.
That means maceration in fresh water. The study is important because it is based on both a good skeletal sample of fetuses (244 males and 212 females) and on Indian population. It is difficult to construct fetus skeletal collections of this size and, because of this, there is a great lack of documented (known sex and age) skeletal collections of individuals at this stage of development. In turn, this lack of fetus skeletal documented collections makes it difficult to develop skeletal growth studies on this age group, which are extremely necessary in forensic and archaeological anthropology, because they help us to estimate fetal age in cases where a perinatal or fetal individual is involved. The paper presents a new documented fetal skeletal collection, an Indian collection, and furnishes information on skeletal growth of Indian fetuses, which is extremely important for osteological research, and population variability.
Very extensive studies have been carried out, in respect of growth on infants and children (Tsuzaki et al., 1990; Shimura et al., 2005; Smith, 2007; Cardosa et al., 2014; Irurita et al., 2017), children through adolescence (Kulkarni, 1985; Padmanathan et al., 1990; Beunen et al., 1990), and also adults (Munoz et al., 2001; Mahakkanukrauh et al., 2011; Wang et al., 2012). Studies are also available on the growth aspects of human in their intrauterine life on the basis of osteometric analysis (Simon et al., 1984; Huxley, 1998; Loughna et al., 2009; Carneiro et al., 2013; Bartosch et al., 2019). Although various studies are available on fetal growth and development, the aims of these studies vary from one another. More studies aimed to concentrate on developmental aspects rather than growth aspects based on osteometry (O’Rahilly, 1973; Kulkarni et al., 1981; Mahon et al., 2009). Several studies have established an association between gestational age and the diaphyseal length fetal long bones (Fazekas and Kosa, 1978; Carneiro, 2019). Studies are available to estimate fetal age from the diaphyses of long bones (Mehta and Singh, 1972; Vare and Bansal, 1977; Kosa, 1997; Shirley, 2009). The estimation of fetal age is applicable in clinical, forensic and archaeological contexts (Butt and Lim, 2014; Carneiro et al., 2013).
The methodology adopted in the earlier studies to prepare the fetal material in dealing with prenatal growth and development was not uniform. In some studies (Ford, 1956; Mehta and Singh, 1972), fetal bones were dissected from preserved fetuses and measured. In the case of measurements taken on the dissected bones, not only would there be every chance of tender fetal long bones getting damaged, but also the removal of soft tissues from the bones might not be that perfect, which might result in distorted measurements. Moore and Persaud (1993) measured human fetuses which were preserved in formalin. Moss et al. (1955) studied fetal bones prepared with alizarin staining. Measurements on long bones, which were obtained from chemically preserved fetuses, definitely differ from that of original long bones.
Therefore, it is necessary to prepare original bone and take measurements directly on the bone to get accurate results. In various studies, observations and measurements were taken from just photographs (Burdi, 1969), radiographs (Piercecchi-Marti et al., 2002; Khan and Faruqui, 2006; Carneiro et al., 2019) and ultrasonographs (Chitty and Altman, 2002; Loughna et al., 2009; Butt and Lim, 2014). The methodology adopted by the earlier workers to measure fetal bones from photographs, radiographs and ultrasonographs might not be accurate, as there was every chance of bones being oblique in their exhibits. Moreover, the bone measurements taken from these graphs showed only a one-dimensional approach, while the bone itself exhibited a multi-dimensional form. While commenting on measurements taken from the ultrasonographs, Chitty and Altman (2002) pointed out that the measurements would vary over a wide range due to differences in fetal position, and difficulties would occur in taking correct linear measurements because of variation of objective planes due to the movements of the fetuses. Moss et al. (1955) studied fetal bones prepared with alizarin staining. In some other studies (Ford, 1956; Mehta and Singh, 1972), fetal bones were dissected from chemically preserved fetuses and got measured. Chemical preservation results to shrinkage of specimens to some extent. Mehta and Singh (1972) measured the crown-rump length of fetuses, after fixing them in 10% formalin for 4 to 6 months. Thus, it is revealed that no uniform method has been adopted in the earlier studies in preparing the fetal specimens.
The number of fetal specimens considered in the earlier studies also varied from one another. It has been noted that in many cases the number has been found to be quite inadequate. Gray and Gardner (1969), and Gardner and Gray (1970) studied a series of only 40 embryos and fetuses. Mehta and Singh (1972) measured the diaphyseal lengths of only 50 fetuses. Dhawan et al. (2014) measured femur bones from 45 human fetuses. Carneiro et al. (2019) measured fetal bones from only 17 fetuses. Because of the inadequacy as well as variability in the sample size, no proper comparison could be made between studies. Most of the earlier studies, which were aimed to estimate age from fetal long bones, did not include all the long bones (Feltz, 1954; Moss et al., 1955; Gray and Gardner, 1969; Gardner and Gray, 1970; Mehta and Singh, 1972).
Going through the literature, it was revealed that there were different aims for the earlier studies. There were variations in methodology adopted to make the availability of the human specimens and also to measure them. There was a lesser number of parameters reported on small sample size. Thus, the whole scenario showed an incomplete picture. Thus, it was felt necessary that a systematic study be undertaken to rectify the pitfalls highlighted above. The present work aimed to study the growth pattern and the rate of growth of the fetal radius with side and sex differences, and to estimate crown-rump length (CRL) and crown-heel length (CHL) from the radius, and also to examine the applied significance based on the osteometry on fetal radius.
MATERIAL AND METHODS
Source of fetus
The principal author “(D.S.)” of the paper was an Anatomy staff member in the Department of Anatomy, B.J. Medical College (BJMC) with its attached Sassoon General Hospitals, Pune, India during 1978 to 2011. The Deans of the BJMC and Sassoon General Hospitals, and the Heads of the Department of Anatomy, BJMC were supportive for the collection of human fetuses from the Sassoon General Hospitals. The Professors and Heads of the Departments of Obstetrics and Gynaecology and Forensic Medicine, BJMC, were also cooperative to supply the human fetuses from their respective departments. The fetuses were collected during the above period. The fetuses were from abortions of Medical Termination of Pregnancies (MTPs)/Still Births. Fetus collections procedures include such as anatomy departmental assistants to be allotted to collect fetuses, proper labeling of particulars on the fetus containers, issue and receipt of related documents of fetus, etc. The study was conducted in the Department of Anatomy, BJMC. Required approval was obtained from the Ethical Committee of BJMC.
Population base
Anatomical study on humans is both on an individual basis and population-oriented. In the present study, name of the parents of the fetuses and their place of living indicated that all the parents of the fetuses belonged within the geographical area of Maharashtra, India. This broad population base of Maharashtra provided a vital significance, indicating that the fetuses belonged to the Maharashtra population of India.
In all, there were 912 (left- and right-side bones) diaphyses of fetal radius bones from 456 normal human fetuses included for the present study. Among the 456 fetuses, 244 (53.51%) fetuses were males and 212 (46.49%) fetuses were females. The fetuses which were selected for the present study were of varying sizes ranging from 51mm to 394mm in crown-rump length (CRL) with 70 mm to 577 mm in crown-heel length (CHL). The exact gestational age (GA) of the fetuses was not known. Some of the details, such as regarding the LMP (last menstrual period), given by the mothers of the fetuses could be misleading, as many of them want to keep their anonymity, as abortions do not enjoy much social acceptance. Therefore, in the present study, the fetuses were categorized on the basis of the CRL and CHL. As there is earlier literature available to estimate fetal age from the CRL as well as the CHL, this study adopted the already established scales, (Davies 1967; Okajima 1975; Williams and Warwick 1980), to estimate fetal age based on the CRL and CHL. Osteometry was carried out on all the 912 radius bones.
In spite of such a large collection of 456 fetuses, there existed obvious biases in the distribution of samples when individual group and sex were considered. Ideally, a trimester-wise grouping would have given better room for tracking the growth pattern. However, that would leave with only two such trimesters with meaningful sample sizes for comparison, leaving quite a few sample sizes in the remaining groups. Further, the results would provide us room only for a broad growth pattern or generalization. As a via media, an eight-week grouping was adopted, to make a total of four groups. In this way, we can justify the sample size under each group. Here too, although there existed an internal biasness in the distribution of sex-wise sample size in the group I, the remaining three groups showed good consistency in the sex-wise distribution of sample. For the purposes of discussion, the assigned group numbers, i.e. I, II, III and IV, would be used throughout this paper. All the 456 fetuses were categorized into four age groups, each group having eight weeks of duration of age range, except for the first group (Table 1). The first group had only a six-week range, because fetal bones would be available for manual measurements only after the period of 11 weeks of the intrauterine development.
Somatometry
When a fetus was brought to the Department of Anatomy, it was to be prepared for somatometric measurements. Only those fetuses that appeared normal were selected for the purpose of the present study. Firstly, the umbilical cord of the fetus was tied tightly with the help of a thread, near the umbilicus. The purpose of the tying up was to stop oozing out of the fetal blood from the fetus. The part of the umbilical cord along with the placenta was cut off and removed. The fetus was then cleaned with running water for about few minutes and kept ready for observation and taking somatometric measurements. The sex of the fetus was noted down. There were two somatometric measurements, CRL and CHL, selected for the present study. After the completion of the somatometry, the fetuses were kept for natural maceration process for the preparation of the fetal bones. No chemical was used in the maceration process.
Osteometry
There were seven osteometric measurements (Table 2) taken on the diaphyses of the fetal radii (Fig. 1) for this study. All the seven osteometric measurements were measured on both right and left bones. The maximum length of the radius is the maximum straight-line distance between the highest point on the proximal end and the lowest point on the distal end of the radius. The remaining measurements were taken at the proximal/distal/middle part of the radius from the maximum straight-line distance from anterior/posterior/medial/lateral-most points as per the name of the measurement. Except the length of the radius (in this study called r-ml) and the midshaft transverse diameter (in this study called r-mml), the remaining five measurements were newly introduced in this study.
Table 2. Osteometric measurements on fetal radius.
|
S.No. |
Osteometric Measurement |
Abbreviation |
|
1 |
Radius-Maximum Length |
r-ml |
|
2 |
Radius-Proximal Antero-Posterior Diameter |
r-pap |
|
3 |
Radius-Proximal Medio-Lateral Diameter |
r-pml |
|
4 |
Radius-Distal Antero-Posterior Diameter |
r-dap |
|
5 |
Radius-Distal Medio-Lateral Diameter |
r-dml |
|
6 |
Radius-Middle Antero-Posterior Diameter |
r-map |
|
7 |
Radius-Middle Medio-Lateral Diameter |
r-mml |
Statistical considerations
Regression coefficient
It was calculated using the following formula.
ΣX ΣY
ΣXY - --------------
N
byx = ----------------------------------------------
(ΣX)2
ΣX2 - --------------
N
Where, byx = regression coefficient of dependent variable Y (e.g., r-ml) on independent variable X (CRL/CHL). In the present study b0 and b1 were used in places of by and bx.
Tests of significance
t-test: The computation of values of ‘t’ was according to the given formula.
Where, X1 and X2 = mean of sample 1 and 2 respectively, and
S.E. X1 and S.E. X2 = standard error of mean of sample 1 and 2, respectively. The value of ‘t’ obtained was checked against the total degrees of freedom to get the level of significance (Singh and Bhasin, 1989).
The degrees of freedom used were obtained by using the following formula.
d.f = ( N1 + N2 ) – 2
where, N1 and N2 = total number of sample 1 and 2, respectively.
Absolute growth rate calculation
For calculating the absolute growth rate based on all the present measurements, the following formula (Biswas and Bhattacharya, 1966) was followed.
Absolute growth
---------------------
S1
Absolute growth rate
percent per month = ------------------------ x 100
N
Absolute growth = S2 – S1
S1 = mean of the maximum length of the radius within the group I
S2 = mean of the maximum length of the radius within the group II
Thus, the absolute growth for the inter-group I and II was the subtraction of the mean growth of group I from the mean growth of group II.
Length of period (N) for the present study is two-month duration.
Accordingly, the inter-group-wise absolute growth rate was calculated for the present study as absolute growth rate percent per month.
RESULTS
Side differences
Side differences (Tables 3 and 4) were analyzed on all the group-wise radius bones of the present study on the basis of the osteometric measurements. In the males, significant left-side dominance was observed from the group II in the r-pml at 1% level and in the r-dap at 5% level. Also in the males, the r-pml showed significant left-side dominance at 5% level from the group III. In the case of females, the r-pap and the r-map showed significant left-side dominance at 5% level from the group III. Also in the females, the r-ml showed significant right-side dominance and the r-pml showed significant left side dominance and both the latter r-ml and the r-pml were at 1% level from the group II. And also in the females, the r-dml showed significant right-side dominance at 5% level from the group III and significant left-side dominance at 5% level from group IV. On the basis of the analyses, it was observed that only 8.04% showed significant side differences in the osteometric measurements (Table 5).
Sex differences
Sex differences were analyzed on all the group-wise radius bones of the present study on the basis of the osteometric measurements (Table 6). Significant sex differences were found between the males and females in the r-mml at 5% level from group I; In the r-pap, r-pml, r-dml at 5% level and in the r-map, r-mml at 1% level from group II; In the r-mml at 5% level from group III. In all these measurements, the females showed higher values. On the basis of the analyses, it was observed that only 12.5% showed significant sex differences (Table 7).
Growth rate
From the regression values (b0, b1) calculated for the osteometry, all the osteometric measurements showed an increasing trend of growth rate for every 1 mm increase in CRL and CHL. The b1 values showed (Tables 8 and 9) increase in the osteometric measurements for every one mm increase in CRL/CHL. Among all the measurements, the r-ml showed faster rate of growth both in the males and females. The fastest rate of growth was observed in female radius from the group I (11 to 16 weeks). For every 1 mm in the CRL, the r-ml was increased by .235 mm. In the group I (11 to 16 weeks), mostly the females showed slightly higher values in almost all the osteometric measurements than the males. In all the osteometric measurements, in both the males and females the group II (17 to 24 weeks) showed slightly higher rate of growth when compared to the group III (25 to 32 weeks). The growth rate of r-ml was higher in the group I compared to the group IV in both the males and females.
Absolute growth rate
The absolute growth rate percent per month for the male and female fetuses belonged to the inter-age group I, II and III were calculated (Table 10). The r-ml of males from the inter-age group I-II (11 weeks to 24 weeks) showed the highest absolute rate of fetal growth as 70.25% per month. The lowest absolute growth rate was found in the r-ml of females from the inter- age group III-IV (25 weeks to 40 weeks) as15.01% per month. Absolute growth rate for the r- ml was higher in the inter-age group I-II (11 weeks to 24 weeks) and gradually declining through the proceeding two inter-age groups II-III (17 weeks to 32 weeks) and III-IV (25 weeks to 40 weeks) (Fig. 2).
Bivariate distribution
In the case of osteometry, variations between the CRL with the r-ml were computed. Because of the smaller sample size in the groups I and IV, scatter diagrams were prepared only for the groups II and III. The scatter diagrams (Figs. 3 and 4) showed that there were very close relationships found between the CRL with r-ml. The obtained scatter diagrams showed a good fit between the variables correlated.
Correlations
In the present study, there were highly significant correlations obtained between the CRL/CHL with all the osteometric measurements (Table 11). In the males, the highest value of correlation coefficient .992 at 1% level as found between the CRL and r-ml in the group I. In the females, the highest value .977 at 1% level was found in between the CHL and r-ml in the group II.
Age estimation of human fetus
As there were highly significant correlations obtained between the CRL/CHL with all the osteometric measurements, necessary regression equations were calculated to calculate the CRL and CHL from all the osteometric measurements (Tables 12 and 13). Necessary regression values (b0, b1) were calculated for the osteometric measurements for age estimation. With the help of the tables 12 and 13, the CRL and CHL can be calculated using the two values b0 and b1 and given measurements. Once the CRL/CHL was calculated, the fetal age could be estimated from the already established age estimation scale.
The formula to calculate CRL/CHL is as follows:
CRL/CHL = (b1 × measurement on the radius) + b0
DISCUSSION
Side and Sex differences
The side differences in the considered measurements indicated certain specific trends that might reveal side dominance. However, there being a low percentage (8.04%) of significant side differences, in the present study all the analyses including the mean and standard deviations, correlation coefficients, regression analyses, analyses on growth and age estimation were calculated on the basis of the mean values of both the left and right sides merging together. In the case of sex differences, in spite of the very low percentage (12.5%), in the present study all the obtained results on correlation coefficients, regression constants for growth rate and also scattergrams along with regression fit lines and bar diagrams were presented sex-wise separately for evolving a broad comparative perspective on both sexes.
Table 12. Regression values (b0, b1) for estimating CRL, from radius from the total sample of 456 fetuses.
|
Osteometric measurements on Radius |
Group –All |
|
|
b0 |
b1 |
|
|
r-ml |
16.964 |
5.890 |
|
r-pap |
24.464 |
57.889 |
|
r-pml |
23.237 |
55.199 |
|
r-dap |
45.795 |
44.009 |
|
r-dml |
46.668 |
32.504 |
|
r-map |
19.278 |
104.106 |
|
r-mml |
26.585 |
85.733 |
Table 13. Regression values (b0, b1) for estimating CHL, from radius from the total sample of 456 fetuses.
|
Osteometric measurements on Radius |
Group –All |
|
|
b0 |
b1 |
|
|
r-ml |
24.491 |
8.807 |
|
r-pap |
36.628 |
86.215 |
|
r-pml |
35.162 |
82.080 |
|
r-dap |
68.524 |
65.501 |
|
r-dml |
69.933 |
48.350 |
|
r-map |
28.526 |
155.294 |
|
r-mml |
39.894 |
127.623 |
Growth rate
Studies on bone growth, based on quantitative analyses, enable a better understanding of the growth pattern. On the basis of the analyses on osteometry, the present study revealed that there was a positive growth trend, which was observed in all the measurements taken on the fetal radius from all the four age groups considered. Moss et al. (1955) stated that several combinations of osseous shaft lengths revealed a constant ratio between the specific growth rates of all the bones. They measured 106 fetuses, which were cleared and stained with alizarin, ranging from 30 mm to 169 mm in CRL, whereas in the present study in the same age group (I and II), 333 fetuses got measured. The present osteometric study was carried out on 912 naturally macerated, dried bones from 456 fetuses. Variations observed with the earlier results (Table 14) might be attributed to the very low sample size of the earlier studies and the mode of preparation of the bone material for the osteometric study. Moss et al. (1955) noted a characteristic interphase in the growth of the body shaft in the CRL interval of 80 - 89 mm. Before the interval, the body shafts of all the long bones grew relatively faster than the CRL, and after that the growth rate was not as fast as it was before. Fazekas and Kosa (1966a, b) determined the size of embryos from the dimensions of the radius. In the present study, measurements on fetal radius have been correlated with the CRL and CHL for fetal age estimation. Fazekas and Kosa (1966a, b) in an attempt calculated the mean lengths of all six limb bones at two weeks intervals from 12 to 40 weeks, whereas in the present study the fetuses were categorized with eight-week intervals, except for the first group which had a six-week interval. Vare and Bansal (1977) observed a linear correlation between the diaphyseal length of the upper and lower limbs and the CRL from 185 fetuses of 116 males and 69 females with CRL ranging from 185 - 415 mm. The bones were dissected from the body and got measured. Although the muscles and connective tissue were removed from the bones, the periosteum was left intact. Vare and Bansal (1977) reported about all the long bones except the clavicle. In these studies, the calculation of growth rate was found not on the basis of age groups, whereas in this study the growth rate was calculated using regression equations, in all the four age groups under the male and female categories separately for all the osteometic measurements. Thus, in this study a broad understanding was evolved on the growth rate of fetal long bones, age-wise and sex-wise. Vare and Bansal (1977) reported that for every 1 mm increase in CRL the length of radius increases by 0.15 mm, whereas the present study reported that the groups I, II, III and IV showed 0.188 mm, 0.187 mm, 0.110 mm and 0.149 mm respectively in the males and 0.235 mm, 0.183 mm, 0.137 mm and 0.150 mm respectively in the females.
Table 14. Mean of Maximum Length of Radius (r-ml): Comparison.
|
Group I |
Group II |
|||
|
Bones |
Moss et al. (1955) |
Present study |
Moss et al. (1955) |
Present study |
|
Radius |
7.80 |
11.20 |
22.32 |
24.14 |
Absolute growth rate
As there were four age groups viz. I, II, III, IV, the absolute growth rate was calculated between these four groups. Thus, there were three inter-age groups formed from the four basic groups as I-II, II-III, and III-IV. Each inter-age group had the total number of fetuses from both the groups concerned. The absolute growth rate was calculated only for the r-ml for the present study. The bar diagram (Fig. 2) revealed the absolute growth rate for the r-ml of both the males and females between the three inter-age groups. Thus, the prepared bar diagram not only helps understand the trend of absolute growth rate but also shows sex differences.
Age estimation
As the CRL and CHL were found closely correlated with all the osteometric measurements, it showed that that a clear dynamic relationship existed between the CRL/CHL with all the osteometric measurements. Expert opinion is routinely requested from anatomists, by legal authorities, to know about the age and sex of the deceased, while dealing with suspected murder cases. While examining the adult cases, as there are already established scales available for age estimation, it becomes easy to estimate the age of deceased adult individual from the bone remains. On the contrary, when opinion about the age of a deceased fetus is asked from the available fetal bones, as there is no established scale or standards available, even anatomists are not in a comfortable position to provide precise information regarding the age of fetus from the bone remains. Mehta and Singh (1972), Vare and Bansal (1977) and Fazekas and Kósa (1978) measured fetal long bones, which include the radius, from a radiographic sample. Kosa (1997) attempted to estimate fetal age from the chemically preserved fetal long bones. Simon et al. (1992), Simon and Baig (2015a, b) and Simon et al. (2020a, b) estimated CRL/CHL from the clavicle, humerus, femur, tibia and fibula respectively, and these studies were carried out on naturally macerated fetal bones without adding any preservative. This study emphasizes that definitely there is variation between taking measurements from radiographs, ultrasonographs, photographs and bones from chemically preserved fetuses and taking measurements directly from the naturally macerated bones. In this study, once the CRL/CHL is calculated from the analyzed regression values based on the osteometry on fetal radius bones, age can be estimated from the already established age estimation scale.
Applied significance
The applied significance in the clinical aspects in this study would enable us to advance a standard, which would help comprehend the differential growth pattern between normal and abnormal fetuses. The analysis in the present study to estimate fetal age from the measurements on the human fetal radius bones would definitely help in solving problems facing the estimation of fetal age, a crucial factor in medico-legal cases. The anatomical aspects of this population-based study on growth pattern in relation to age and sex variations would open new vistas for research in the field of fetal growth.
Related articles


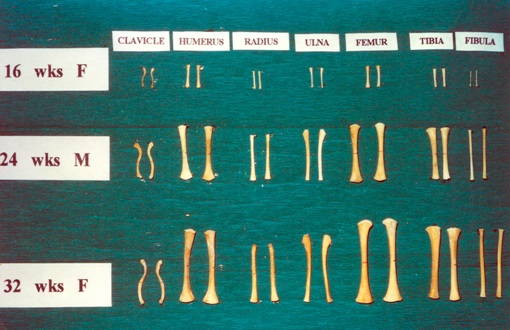 Fig. 1.- Shafts of fetal long bones (16 to 32 weeks) (Sample).
Fig. 1.- Shafts of fetal long bones (16 to 32 weeks) (Sample). 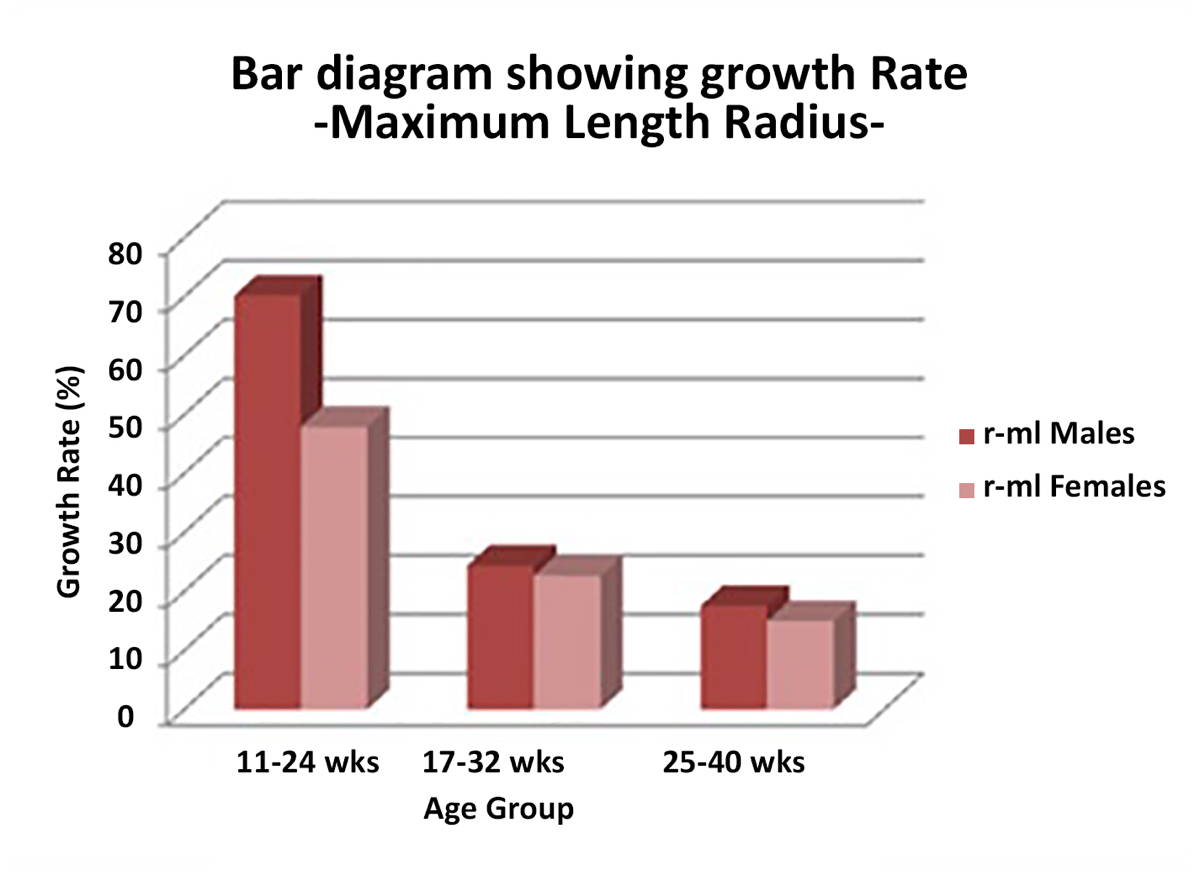 Fig. 2.- Absolute growth rate of fetus based on maximum length of radius.
Fig. 2.- Absolute growth rate of fetus based on maximum length of radius.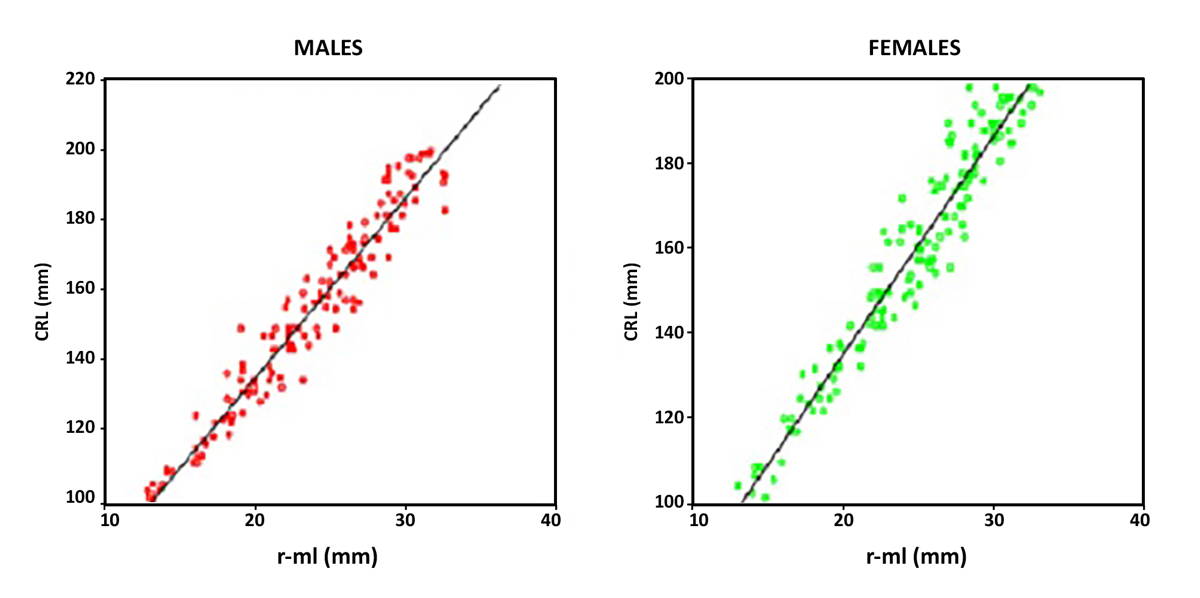 Fig. 3.- Scatter diagrams and regression fit lines for r-ml (mm) with CRL (mm) in Group II.
Fig. 3.- Scatter diagrams and regression fit lines for r-ml (mm) with CRL (mm) in Group II. 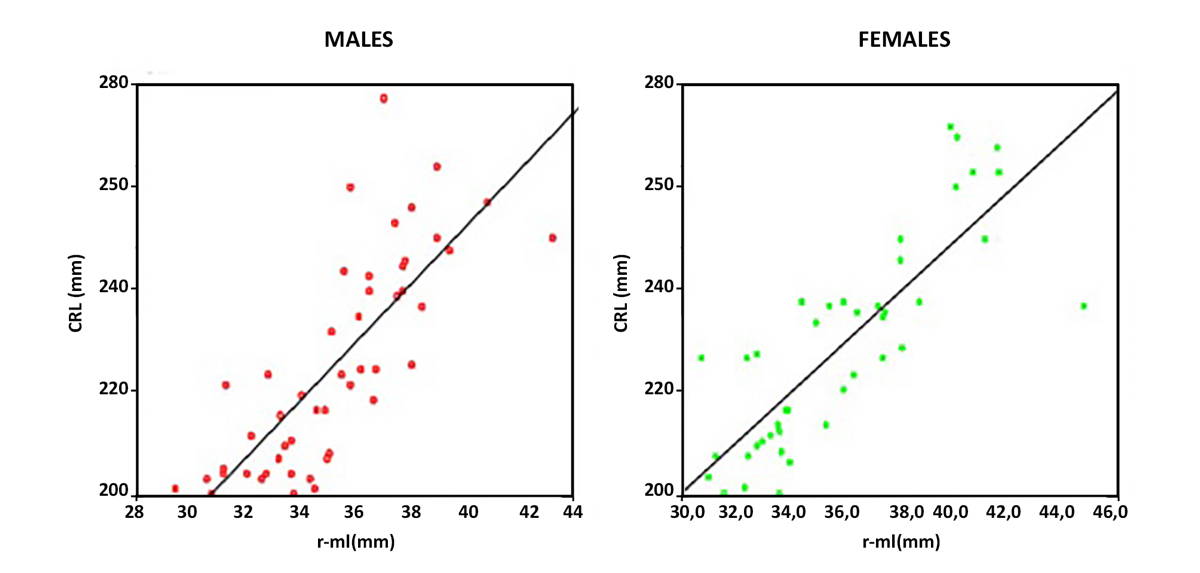 Fig. 4.- Scatter diagrams and regression fit lines for r-ml (mm) with CRL (mm) in Group III.
Fig. 4.- Scatter diagrams and regression fit lines for r-ml (mm) with CRL (mm) in Group III.BARTOSCH C, VILAR I, RODRIGUES M, COSTA L, BOTELHO N, BRANDAO O (2019) Fetal autopsy parameters standards: biometry, organ weights, and long bone lengths. Virchows Arch, 475(4): 499-511.
BEUNEN G, LEFEVRE J, OSTYN M, RENSON R, SIMONS J, VAN GERVEN D (1990) Skeletal maturity in Belgian youths assessed by the Tanner-Whitehouse method (TW2). Ann Hum Biol, 17: 355-376.
BISWAS PC, BHATTACHARYA DK (1966) Growth trends in Northern Indian population variation of four anthropometric traits from birth to maturity. In: Malhotra MS (editor). Human adaptability to environments and physical fitness. Defence Institute of Physiology and Allied Sciences, Madras, pp 270-280.
BURDI AR (1969) Cephalometric growth analysis of the human upper face region during the last two trimesters of gestation. Am J Anat, 125: 113-122.
BUTT K, LIM K (2014) Determination of gestational age by ultrasound. J Obstet Gynaecol Canada, 36: 171-183.
CARDOSO HFV, ABRANTES J, HUMPHREY LT (2014) Age estimation of immature human skeletal remains from the diaphyseal length of the long bones in the postnatal period. Int J Legal Med, 128(5): 809-824.
CARNEIRO C, CURATE F, BORRALHO P, CUNHA E (2013) Radiographic fetal osteometry approach on age estimation for the Portuguese population. Forensic Sci Int, 10:231(1-3): 397.e1-5.
CARNEIRO C, CURATE F, CUNHA E (2016) A method for estimating gestational age of fetal remains based on long bone lengths. Int J Legal Med, 130(5): 1333-1341.
CARNEIRO C, ALEMAN I, BOTELLA M, CUNHA E (2019) Fetal age at death estimation on dry bone: testing the applicability of equations developed on a radiographic sample. Revista Argentina de Anthropología Biológica, 21(2).
CHITTY LS, ALTMAN DG (2002) Charts of fetal size: limb bones. Br J Obstet Gynaecol, 109: 19-29.
DAVIES DV, editor (1967) Gray’s Anatomy. 34th edn. p 261. Longmans, Green, London.
DHAWAN V, KAPOOR K, SHARMA M, SINGH B, SEHGAL A (2014) Morphometry of fetal femora as an indication of gestational age. Eur J Anat, 18(2): 85-92.
FAZEKAS IG, KOSA F (1966a) Neuere Beitrage und vergleichende Untersuchungen von Feten zur Bestimmung der Korperlange auf Grund der Diaphysenmasse der Extremitatenknochen. Deutsche Zeitschrift gerichtliche Medizin, 58: 14-160.
FAZEKAS IG, KOSA F (1966b) Determination of the size of embryos from the dimensions of the radius. Ann Med Leg Criminal Police Sci Toxicol, 46 (Pt 4): 262-272.
FAZEKAS IG, KOSA F (1978) Forensic fetal osteology. Budapest: Akademiai Kiado.
FELTZ WJL (1954) The prenatal development of the human femur. Am J Anat, 94: 1-44.
FORD EHR (1956) The growth of the fetal skull. J Anat, 90: 63-72.
GARDNER E, GRAY DJ (1970) The prenatal development of the human femur. Am J Anat, 129: 121-140.
GRAY DJ, GARDNER E (1969) The prenatal development of human humerus. Am J Anat, 124: 431-446.
HUXLEY AK (1998) Comparability of gestational age values derived from diaphyseal length and foot length from known forensic foetal remains. Med Sci Law, 38(1): 42-51.
IRURITA OJ, ALEMAN AI (2017) Proposal of new regression formulae for the estimation of age in infant skeletal remains from the metric study of the pars basilaris. Int J Legal Med, 131(3): 781-788.
KHAN Z, FARUQUI NA (2006) Determination of gestational age of human fetuses from diaphyseal lengths of long bones - A radiological study. J Anat Soc India, 55: 67-71.
KOSA F (1997) Determination of body length and age of human foetuses and newborns on the basis of weights of limb bones. Acta Biol Szeged, 42: 225-234.
KULKARNI DS, SIMON D, BHANU BV (1981) Dermatoglyphic study on human foetus. J Anat Sci, 3(Pt 1): 47-52.
KULKARNI VS (1985) Profiles of growth of two Endogamous groups [doctoral thesis]. Department of Anthropology, University of Pune, Pune, India.
LOUGHNA P, CHITTY L, EVANS T, CHUDLEIGH T (2009) Fetal size and dating: Charts recommended for clinical obstetric practice. Ultrasound, 17: 161-167.
MAHAKKANUKRAUH P, KHANPETCH P, PRASITWATTANSEREE S, VICHAIRAT K, TROY CASE D (2011) Stature estimation from long bone lengths in a Thai population. Forensic Sci Int, 210(1-3): 279.
MAHON PA, COOPER C, CROZIER SR, GODFREY KM (2009) The use of 3D ultrasound to investigate fetal bone development. Norsk Epidemiologi,19(1): 45-52.
MEHTA L, SINGH HM (1972) Determination of Crown-Rump length from foetal long bones humerus and femur. Am J Phys Anthrop, 36: 165-168.
MOORE KL, PERSAUD TVN, editors (1993) The Developing Human – Clinically Oriented Embryology. 5th edn. Saunders, Philadelphia.
MOSS ML, NOBACK CR, ROBERTSON GG (1955) Critical development horizons in human fetal long bones. Am J Anat, 97: 155-175.
MUNOZ JI, LINAREZ-IGLESIAS M, SUAREZ-PENARANDA JM, MAYO M, MIGUENS X, RODRIGUEZ-CALVO MS, CONCHEIRO L (2001) Determined long bone length in a Spanish population sample. J Forensic Sci, 46(2): 363-366.
OKAJIMA M (1975) Development of dermal ridges in the fetus. J Med Genet, 12: 243-250.
O’RAHILLY R (1973) Developmental stages in human embryos. Part A. Embryos of the first three weeks (stages 1-9). pp 9-31. Carnegie Institution of Washington, Washington.
PADMANATHAN G, PRAKASH S, CHHIBBER SR (1990) Single occasion means of height and weight of Sri Lankan Tamil children from Jaffna. Ann Human Biol, 17(Pt 2): 107-113.
PIERCECCHI-MARTI MD, ADALIAN P, BOURLIERE-NAJEAN B, GOUVERNET J, MACZEL M, DUTOUR O, LEONETTI G (2002) Validation of a radiographic method to establish new fetal growth standards: radio-anatomical correlation. J Forensic Sci, 47: 328-331.
SCHEUER JL, MUSGRAVE JH, EVANS SP (1980) The estimation of late fetal and perinatal age from limb bone length by linear and logarithmic regression. Ann Human Biol, 7(Pt 3): 257-265.
SHIMURA N, KOYAMA S, ARISAKA O, IMATAKA M, SATO K, MATSUURA M (2005) Assessment of measurement of children’s bone age ultrasononically with Sunlight BonAge. Clin Pediatr Endocrinol, 14(Suppl 24): 17-20.
SHIRLEY NR (2009) Age and sex estimation from the human clavicle: An investigation of traditional and novel methods. A Dissertation presented for Ph.D. Degree to the University of Tennessee, Knoxville.
SIMON D, KULKARNI DS, GORE AP, BHANU BV, PATWARDHAN S (1984) Somatometric study on human foetus. J Anat Sci, 6: 1-6.
SIMON D, DESHMUKH AN, BHANU BV (1992) Age estimation from human foetal clavicle. Med J West India, 20: 58-62.
SIMON D, BAIG MM (2015a) Growth analysis and age estimation of human fetus from human fetal humerus. IJIRD, 4(Pt 5): 142-147.
SIMON D, BAIG MM (2015b) Growth pattern and fetal age estimation from the diaphyseal length of femur. IJIRD, 4(Pt 5): 148-152.
SIMON D, ANNIE V, BISWAJIT B, MONIE S, DON V (2020a) Human fetal growth and age estimation based on osteometry on the diaphysis of fetal tibia. IJIRD, 9(5): 40-48.
SIMON D, BISWAJIT B, MONIE S, DON V, ANNIE V (2020b) Fetal growth and age estimation based on osteometry on the diaphysis of human fetal fibula. IJIRD, 9(5): 49-57.
SINGH IP, BHASIN MK (1989) Anthropometry. Bharti Bhavan, Kamla-raj Enterprises, New Delhi.
SMITH SL (2007) Stature estimation of 3-10-year-old children from long bone lengths. J Forensic Sci, 52(3): 538-546.
TSUZAKI S, MATSUO N, SAITO M, OSANO M (1990) The head circumference growth curve for Japanese children between 0-4 years of age: Comparison with Caucasian children and correlation with stature. Ann Human Biol, 17(Pt 4): 297-303.
VARE AM, BANSAL PC (1977) Estimation of Crown-Rump length from diaphyseal lengths of fetal long bones. J Anat Soc India, 26(Pt 2): 91-93.
WANG YZ, HUANG Y, ZHOU XR, DENG ZH (2012) Stature estimation based on the length of tibia and fibula measured by digital X-ray in Chinese Han teenagers. Fa Yi Xue Za Zhi, 28(6): 413-7,425.
WILLIAMS PL, WARWICK R, editors (1980) Gray’s Anatomy. 36th edn. Churchill Livingstone, Edinburgh.