INTRODUCTION
Pancreatic cancer is a global health problem because of its high mortality. It is the seventh cause of cancer deaths worldwide. Our country, Uruguay, ranks 17th in the World and second in America according to the Global Cancer Observatory (GLOBOCAN, 2018). Although the prognosis of this pathology is generally bad, there are certain determining factors that can modify its result. Among them, the margins of resection stand out (Gockel et al., 2007; Perinel and Adham, 2014; Chowdappa and Challa, 2015; Kanhere et al., 2015; Xu et al., 2017). Local recurrence due to incomplete resection, rather than metastatic disease, is considered the primary reason for the poor prognosis of these patients (Xu et al, 2017). Although a consensus has not been established, total mesopancreas excision or right retro-portal lamina (RRPL) resection is suggested during Cephalic duodenopancreatectomy (DPC) in order to decrease local recurrence, improving patient survival (Gockel et al., 2007; Gaedcke et al., 2010; Perinel and Adham, 2014; Chowdappa and Challa, 2015; Kanhere et al., 2015; Cao et al., 2015; Xu et al., 2017). This explains why the term mesopancreas was coined, analogous to the mesorectum (Gockel et al., 2007; Agrawal et al., 2010; Kanhere et al., 2015; Peparini et al., 2015; Sharma et al., 2016; Xu et al., 2017).
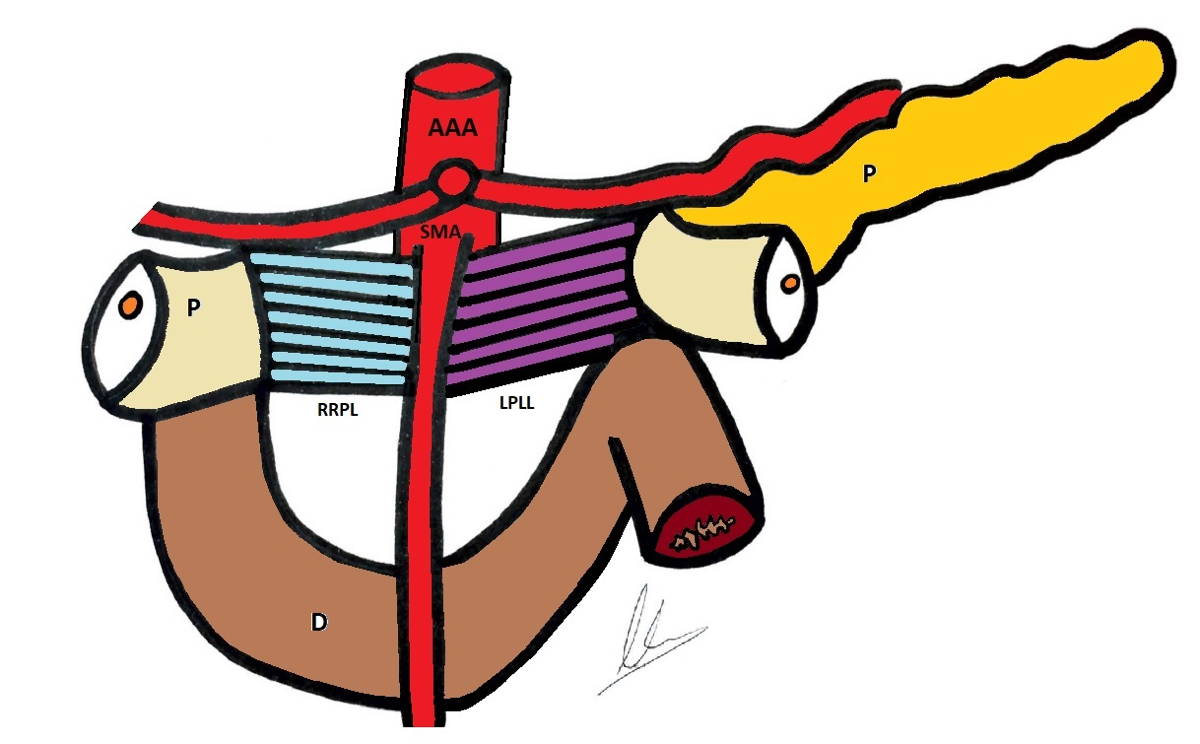
The RRPL also known as right retro pancreatic lamina, was first described by J.B. Prionton and R. Laux in 1959, as a remnant of the pancreas primitive mesodorsal. The pancreas begins its origin in the 4th week of embryonic development from two primordia: dorsal and ventral. The first origins to the left pancreas, body and tail, while the second to the right pancreas: neck, head and uncinate process. Its fusion occurs at the end of the 6th week (Borghi et al., 1998; Skandalakis et al., 2004). Thus, the primitive mesodorsal of the pancreas is composed of two contingents: a left one, known as the left portal lateral lamina (LPLL), and a right one, which corresponds to the RRPL (Fig. 1) (Champetier et al., 1978; Pissas, 1984). Its anatomical description does not appear in classic anatomical textbooks such as Testut (1950), Patel (1957) or Rouviere (1987). According to classic definitions, it is not a true meso, since it does not contain the main vascular-nervous elements of the organ and lacks the characteristic fibrous envelope or fascia that links to the posterior parietal peritoneum (Gockel et al., 2007; Agrawal et al., 2010; Kanhere et al., 2015; Peparini et al., 2015; Sharma et al., 2016; Xu et al., 2017). Recently, a series of studies involving intra-operative, radiological and cadaveric dissections suggested that the idea that regions of mesentery regress may not be accurate (Kumar et al., 2020).
The RRPL is a dense connective tissue formation, with a rectangular shape, whose limits are: pancreas uncinate process (UP) to the right, superior mesenteric artery (SMA) to the left, right celiac ganglion upwards and duodenum third portion downwards. It contains vascular elements: arterial, venous and lymphatic, as well as nerve fibers (Champetier et al., 1978).
The aim of the following work is to perform an anatomical and histological study of the RRPL.
MATERIALS AND METHODS
Thirty adult cadavers of both sexes (10 men and 20 women), between 40 and 90 years old, fixed in formaldehyde-based solution were used. None of them presented previous abdominal surgery.
The cadaveric material was used following the rules of the Helsinki Declaration regarding prior live donation and informed consent, a sine qua non condition for the anatomy department at the Faculty of Medicine in the Universidad de la República.
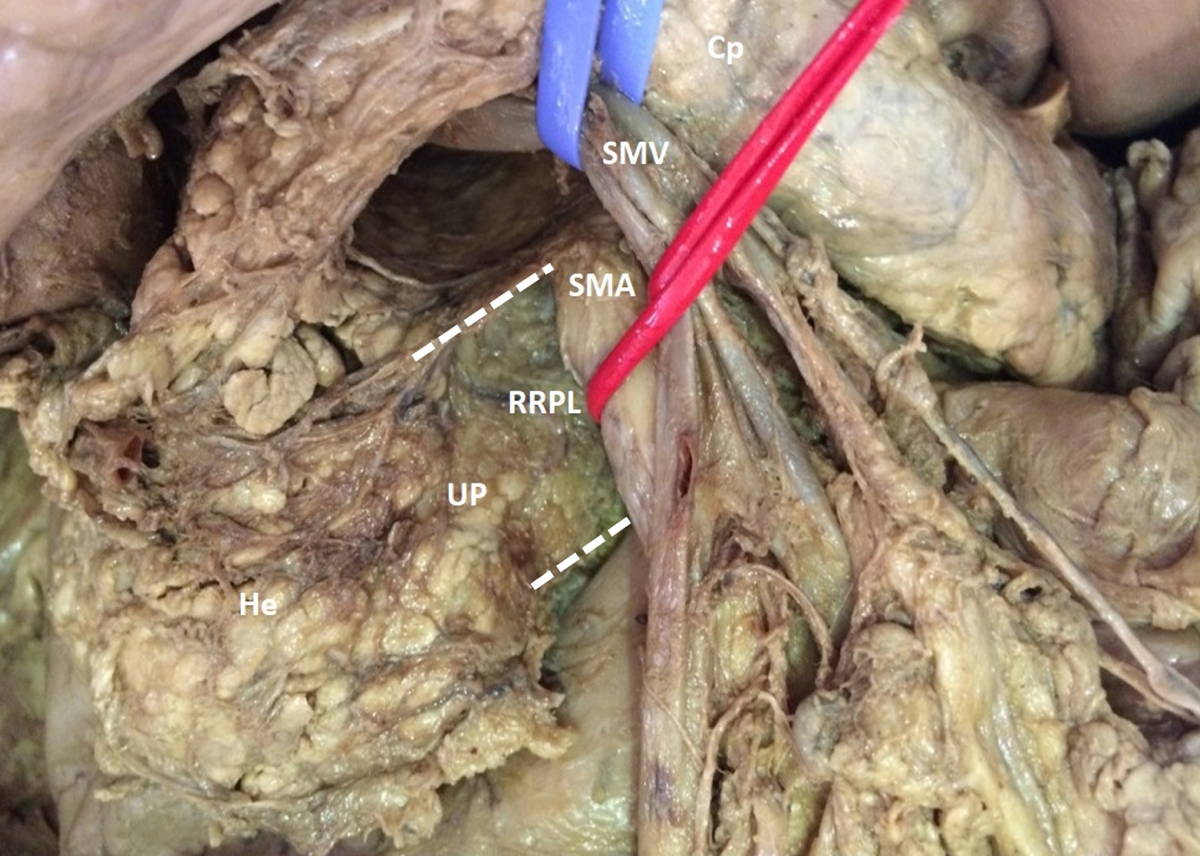
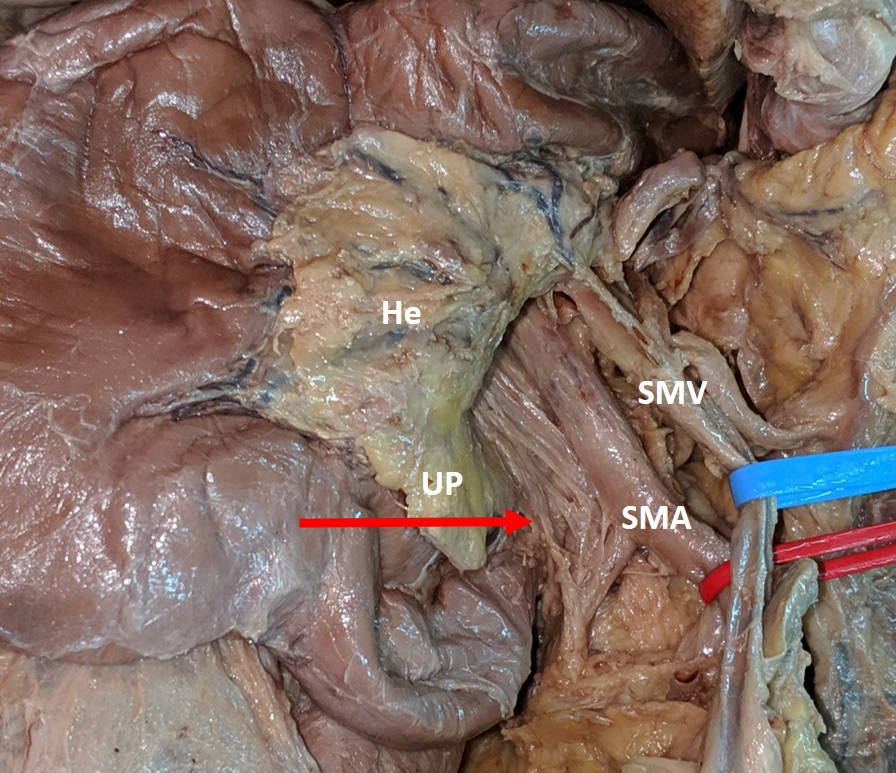
Dissection of the duodenum-pancreas and its main vascular pedicles was performed. A medial xiphopubic incision was made. Once inside the peritoneal cavity, we proceeded to disinsert the grastrocolic omentum from its colic insertion, raising the stomach and descending the transverse colon and mesocolon. Subsequently, the right colic flexure was mobilized medially in favor of the pre-duodenal pancreatic fascia, exposing the pancreas anterior surface. Once the UP was identified, its relationship with the superior mesenteric vessels was assessed, and a careful dissection of the RRPL was made (Fig. 2).
The presence of the RRPL, its limits, dimensions, and macroscopic content were registered. All records were made by the same observer with a digital millimeter gauge.
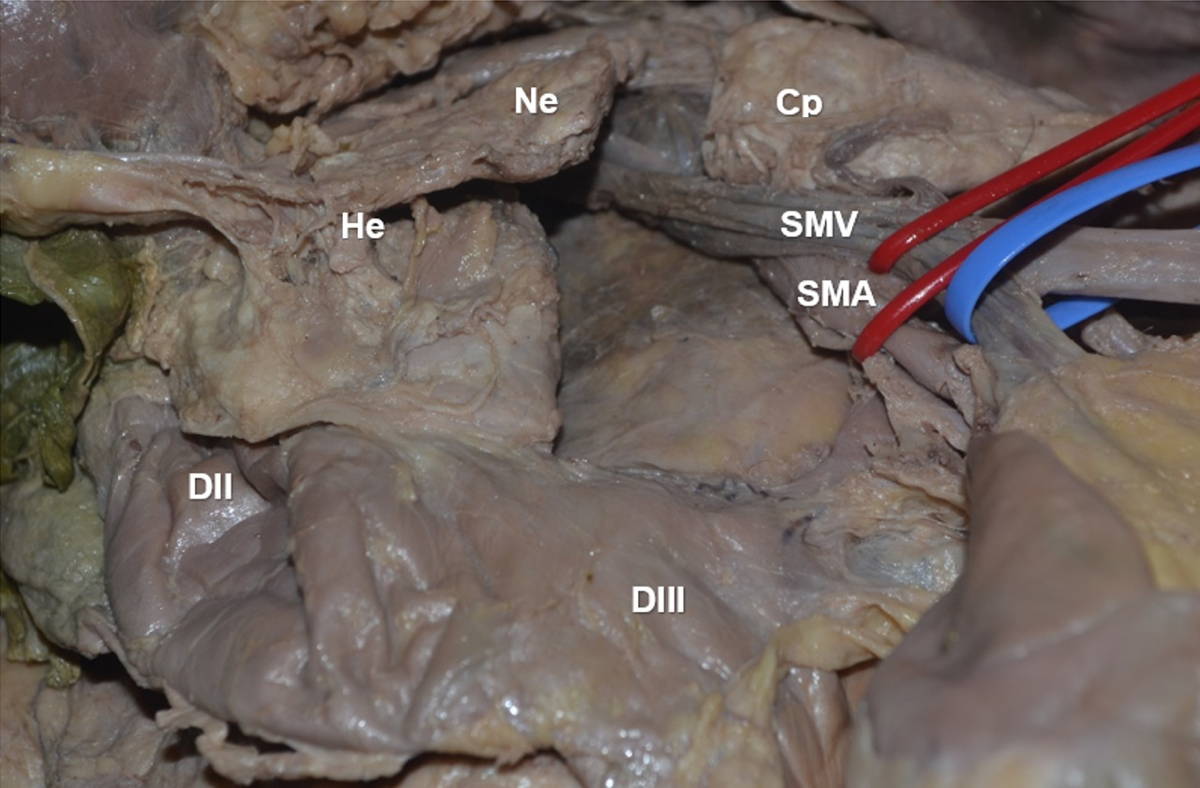
Afterwards, the lamina was resected (Fig. 3 and Fig. 4) and sent to the Histology and Embryology Department. The pieces were embedded in paraffin, and sliced and stained with hematoxylin and eosin. The images were obtained with a Nikon D320 Microscope with digital camera. Microscopic content was registered.
RESULTS
Presence of RRPL, limits and dimensions
The presence of RRPL was found in 100% of the cases (n=30). It extended laterally to the UP (100%, n=30) and medially to the vascular sheath of SMA. We emphasize that at the time of the lamina resection a sub-adventitial dissection of the SMA was needed. Its dimensions were 20 mm long, 17 mm wide and 3 mm thick.
Macroscopic content
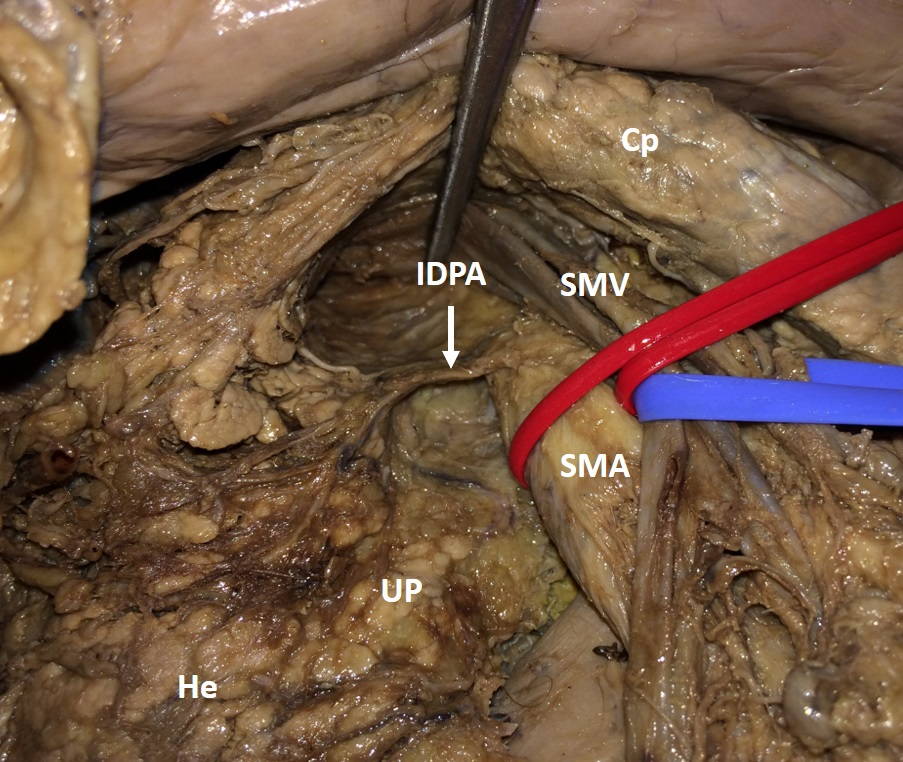
Vascular and nervous elements were found during dissection. Regarding the arterial content, the inferior pancreatic-duodenal artery was identified in 26.6% of the cases, in which the RRPL extended on the right margin of the SMA below its origin (Fig. 5). We also found the presence of small tributary veins of the superior mesenteric vein, such as inferior pancreatic duodenal veins.
The study of the macroscopic lymphatic content was a real challenge. Only in one of the cases did we find macroscopically evident lymph nodes. In that case, the dissection showed the presence of a mass at the cephalo-pancreatic level, suggestive of a cephalo-pancreatic adenocarcinoma, although we did not count with available information to corroborate this hypothesis.
Regarding nervous content, fibers were found entering the medial margin of the UP (Fig. 6), made up of post ganglionic fibers of celiac ganglia, and from superior mesenteric periarterial plexus.
Microscopic content
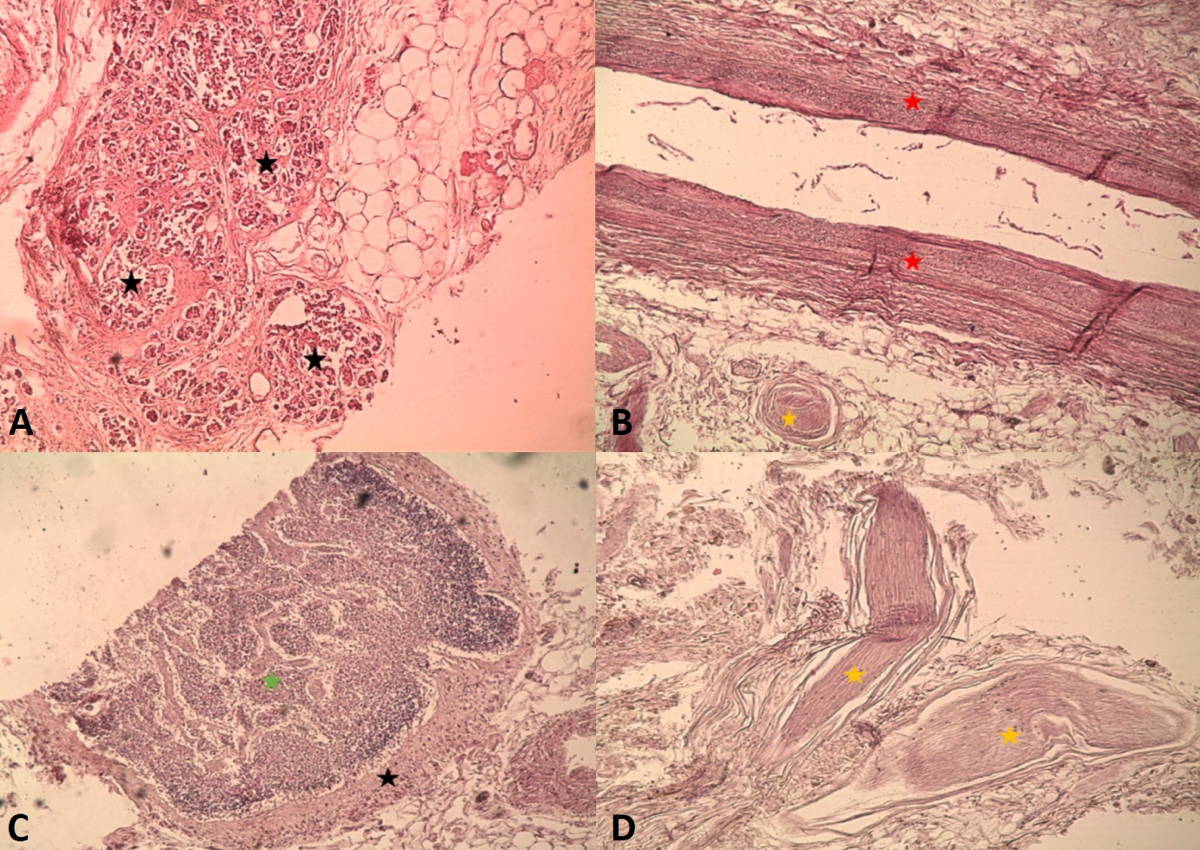
The microscopic study of the lamina confirmed the presence of vascular elements: arterial, venous and lymphatic, as well as nervous fibers. The findings are illustrated in Fig. 6. We highlight microscopic presence of lymphatic content of the lamina, showing vessels and lymph nodes that could not be identified with the naked eye. In addition, pancreatic parenchyma was found on the right margin of the resected laminas (Fig. 7).
DISCUSSION
The RRPL can be identified with relative ease given its constant limits. To the right of the minor pancreas, the parenchymal sector extends from the head of the pancreas to the left behind the superior-portal mesenteric vascular axis. Also called retro-venous pancreas, it can be divided in three parts, from top to bottom: retro-portal, which hints behind the portal vein; retro-mesenteric, located immediately behind the superior mesenteric vein; and UP, which corresponds to the lower portion of the segment with variable extension to the left (Pissas, 1984).
To the left, its limit is the SMA, which requires a sub-adventitial dissection. The superior mesenteric artery originates from the anterior surface of the abdominal aorta, at the level of the first lumbar vertebra, and is directed down and forward obliquely. It originates in its left margin jejunal branches, and in its right margin the inferior pancreatic-duodenal arteries, which run in the thickness of the RRPL and had to be ligated and sectioned at its origin for resection.
As found in our work and in the consulted bibliography, its length ranges from 18.66 mm to 60 mm, a value that depends on the variable extent of the pancreatic parenchyma on the left. Its width and thickness do not exceed 30 mm and 4 mm respectively (Bouassida, 2013).
The content of the RRPL was concordant with the bibliography consulted. The inferior duodenal pancreatic arteries originate from the right margin of the SMA, and run from left to right to the duodenum pancreas. The right hepatic artery, whose incidence has been reported in approximately 14% of cases by different authors, was not found in our work. When present, it originates from the right margin of the superior mesenteric artery, and runs obliquely up and to the right contained in the thickness of the RRPL. Its correct identification and protection are essential in order to avoid catastrophic consequences (Hiatt et al., 1994; Mugunthan et al., 2016).
The dissection of the RRPL shows the presence of small tributary veins of the superior mesenteric vein. Some authors have described the passage of the inferior pancreatic-duodenal veins and small tributaries of the retro-venous pancreas.
The RRPL contains lymphatic vessels of drainage of the UP and posterior surface of the pancreas head, as well as part of the anterior face (Pissas, 1984). Pissas (1984) systematized the lymphatic circulation of the pancreas in two currents on both sides of the superior mesenteric artery that drain the right pancreas and left pancreas respectively. The found lymphatic vessels are part of the right current, although we could not identify its origin, distribution and drainage without the use of staining techniques. This is one of the main weaknesses of our work.
The nervous content is of particular interest. It is made up of post ganglionic fibers of celiac ganglia, superior mesenteric plexus and pre aortic plexus, which enter the medial margin of the pancreas hook. It explains possible perineural dissemination pathways of pancreatic head cancer. Yoshioka and Wakabayashi (1950) systemized the aforementioned fibers for the first time under the name of Plexus Pancreaticus Capitalis. According to the origin of its fibers, it can be divided into two portions: an upper one, unco-lunar lamina from the right celiac ganglion; and a lower one, unco-mesenteric, whose fibers come from the superior mesenteric peri-arterial plexus, included on the RRPL (Yoshioka and Wakabayashi, 1950; Yi et al., 2003).
The microscopic findings are the true witnesses of the content of the RRPL, and are consistent with the consulted literature (Bouassida, 2013; Xu et al., 2017).
In summary, the RRPL is a constant connective-vasculo-nervous formation, which constantly involves the proximal portion of the superior mesenteric artery that requires a sub-adventitial dissection. The fact that it contains vascular and nervous elements argues in favor of its resection so as to avoid local recurrences. The lymphatic circulation identification and dissection with staining techniques is one of the aspects to further research in our line of work.
ACKNOWLEDGEMENTS
We especially want to thank donors and their families for enabling us to conduct this research.