INTRODUCTION
There are two external pudendal arteries (formerly called external shame arteries), superficial (or upper) and deep (or lower), which arise from the medial side of the common femoral artery (Bouchet and Cuilleret, 1996).
The branches of the external pudendal artery (EPA) incidentally supply the penis. The latter is mainly vascularized by the branches of the internal pudendal artery (Droupy et al, 1997). Due to an acquired or congenital cause, the vascularization of the penis can be provided exclusively by the branches of the EPA; in this case, degenerative involvement during a chronic illness or trauma, for example surgical, of a dominant EPA can lead to erection difficulty by reducing the flow of blood in the corpora cavernosa (Macchi et al, 1996).
Anatomically, the EPA has variable but very close relationships with the arch of the great saphenous vein (GSV) (Henriet, 1987). In vascular surgery, the latter is dissected and sectioned as part of surgery for varicose veins of the pelvic limb. Thus, at the time of approaching the femoral trigone or dissecting the butt and trunk of the GVS, the EPA can be ligated with the afferents of the butt or completely severed (Gaye et al, 2016).
In plastic surgery, the flaps based on the superficial EPA have been used in the repair of skin defects of the penis rod after fitting prosthesis, in vulvar reconstruction, and in reconstruction of skin lesions of the hand (Thate et al, 1986; Mayer and Rodriguez, 1991; Abe et al, 1992; George et al, 1996).
There has not been much study on the EPA and data are lacking for the Malian population. We undertook this work with the objective of:
specify the number of the EPA;
describe the variations of origin of the EPA;
and describe the relationship of the EPA with the arch of GSV.
MATERIALS AND METHODS
It was a prospective study carried out at the anatomy laboratory of the Faculty of Medicine and Odontostomatology of Bamako during a period of 20 months going from July 26, 2018 to March 14, 2020. We dissected the external pudendal artery 72 times (36 times on the left and right) in 36 corpses including 29 men and 7 women. We included in this study all fresh corpses bearing no trace of trauma or operative scar in the upper half of the anterior aspect of the thigh. We excluded from this study all corpses showing traces of trauma or operative scar in the upper half of the anterior aspect of the thigh. The dissection was performed at the femoral trigone by making 3 skin incisions. The first, oblique incision extended from the anterosuperior iliac spine to the upper medial part of the anterior aspect of the thigh via the pubic spine. The second vertical incision started from the middle of the first incision to the junction of the upper 1/3 and the lower 2/3. The third, transverse incision passed through the lower end of the previous incision. After these incisions, the skin was peeled off, 3 skin flaps were obtained and folded down inside, outside and above. Then, the subcutaneous cell tissue was dissected for GSV. The latter was dissected with the tributary veins of its butt. The EPA was sought at the saphenofemoral junction and dissected to its origin. The femoral artery and vein were also dissected. After these dissections, the photos were taken with the camera of a Samsung Galaxy J6 + phone. The following parameters were noted: the sex of the cadaveric subject; the dissected side; the number, origin and mode of birth of the EPA, and finally the relationship of the EPA with the butt of the GSV.
The data were entered and analyzed using the Epi info software. A comparison between men and women, and between the left and right sides, was made with the Fischer test.
Concerning the ethical aspect, during this work the respect for the anonymity of cadaveric subjects and the confidentiality of information were required.
RESULTS
Number
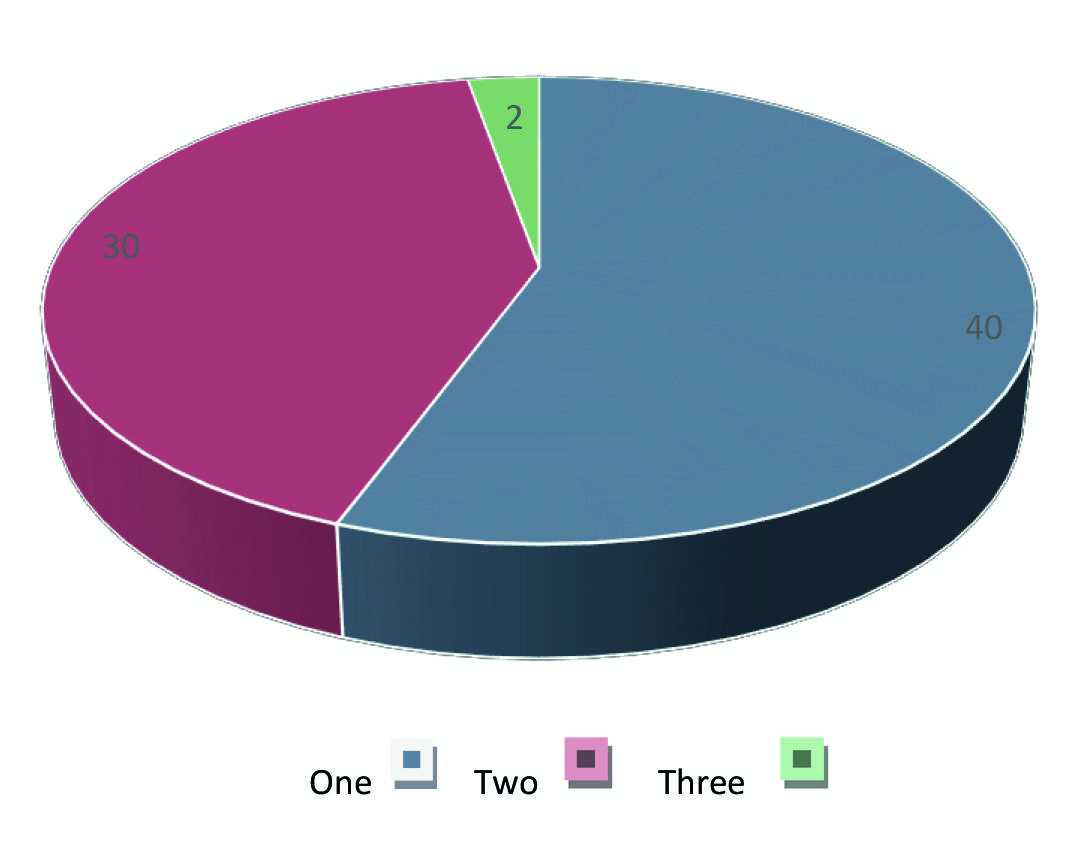
The EPA was visible in all cases. There was only one EPA in 40 cases (55.56%), including 22 cases on the right and 18 cases on the left. According to sex, the presence of a single EPA was observed 33 times in men and 7 times in women. The presence of two APE, superficial and deep, was noted in 30 cases (41.67%); depending on the side, it was observed in 13 cases on the right and in 17 cases on the left; by sex, it was observed in men in 24 cases and in women in 6 cases. In 2 cases, there were 3 EPA, superficial, middle and deep; one case was observed in a man on the right; the other case was seen in a woman on the left.
The difference was not significant between men and women or between the right and left sides, because P>0.05. The number of EPA is summarized in Fig. 1.
Origin
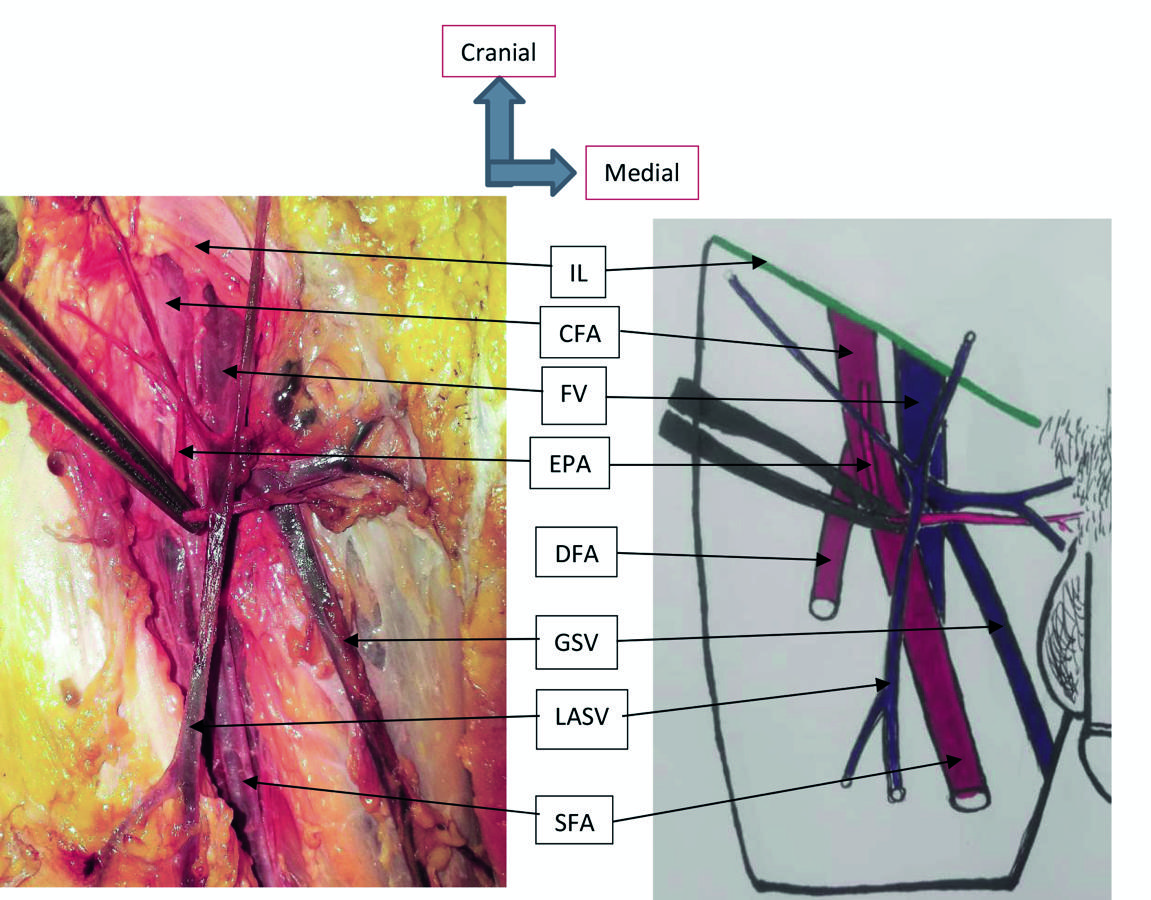
In the 40 cases where there was only one EPA, it came from the common femoral artery (CFA) (Fig. 2) in 18 cases and from the superficial femoral artery (SFA) (Fig. 3) in 22 cases. According to the side, it came from the CFA in 10 cases on the right and in 8 cases on the left; it came from SFA in 12 cases on the right and 10 cases on the left. According to sex, the presence of a single EPA which came from CFA was observed 15 times in men and 3 times in women, the presence of a single EPA which came from SFA was observed 18 times in men and 4 times in women.
In the 30 cases where there were two EPA, we noted 4 types of origin of superficial and deep EPA:
First, the two superficial and deep EPA are both from the CFA. This type of origin was noted in 17 cases. Depending on the side, it was observed in 6 cases on the right and in 11 cases on the left; by sex, it was observed in 13 cases in men and in 4 cases in women.
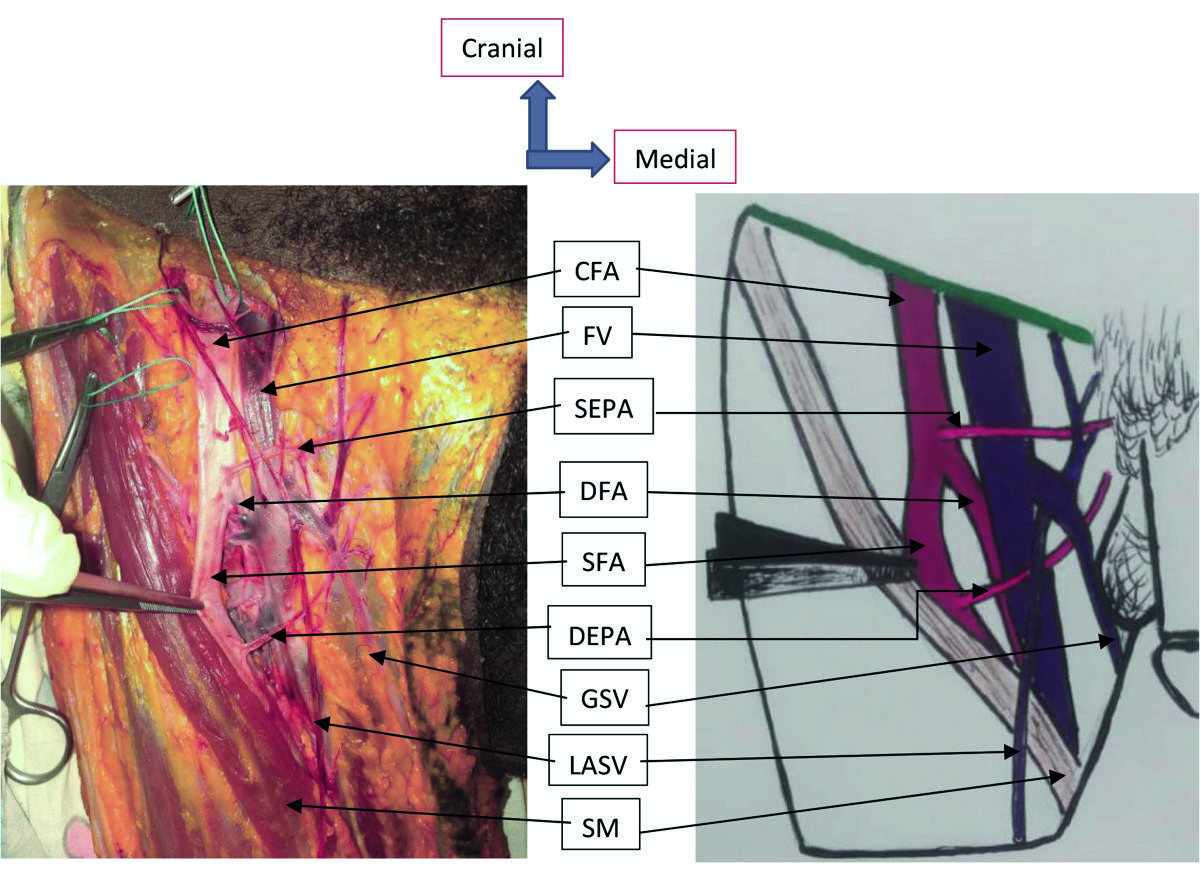
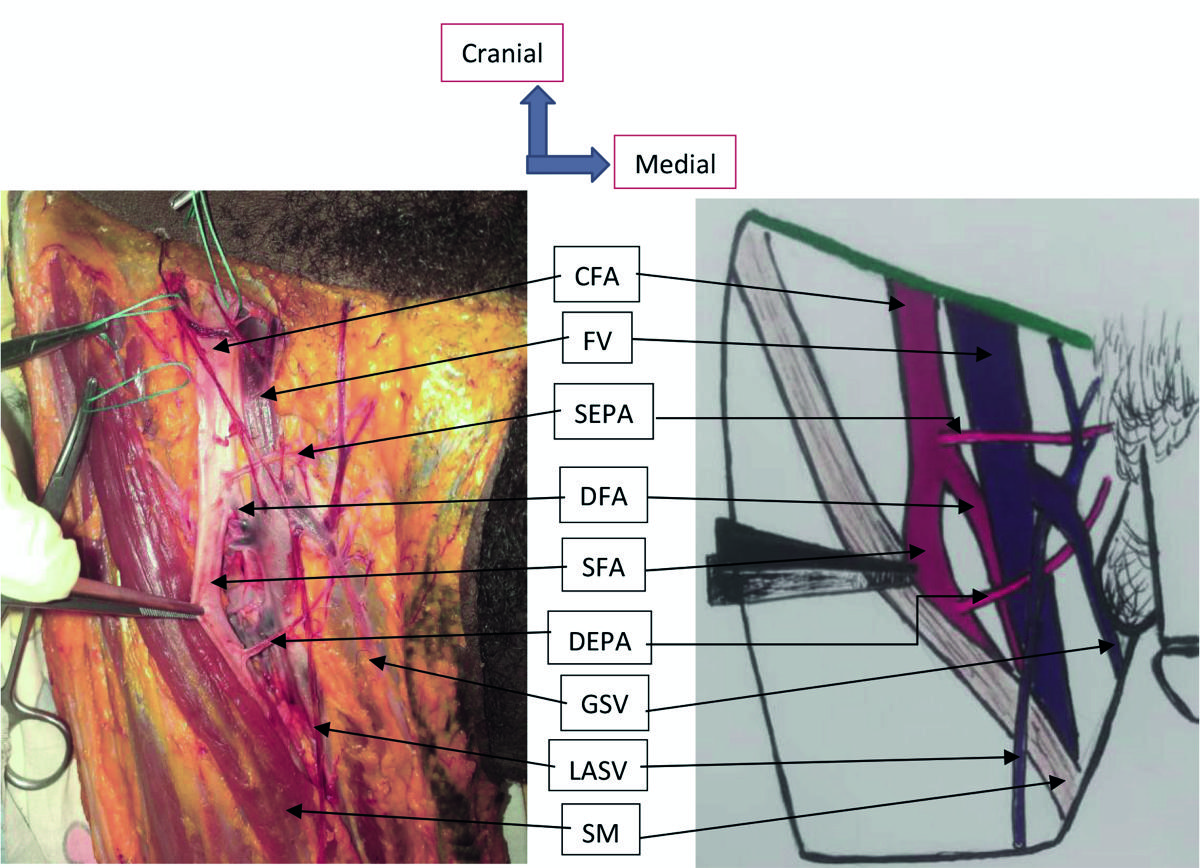
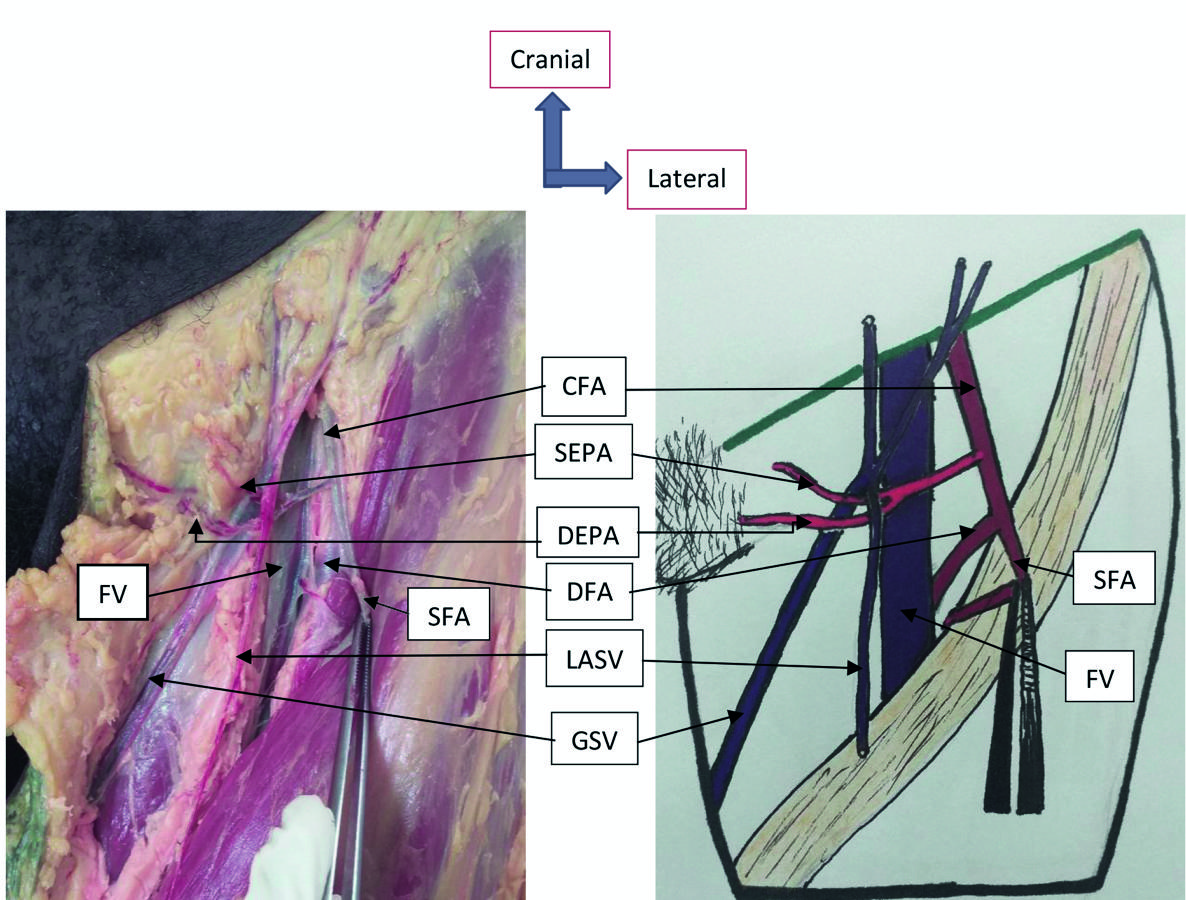
Second, the superficial EPA comes from the CFA and the deep EPA from the AFS (Fig. 4). This type of origin of the EPA was observed in 7 cases. Depending on the side, it was observed in 4 cases on the right and in 3 cases on the left; by sex, it was observed in 6 cases in men and in 1 case in women.
Third, the superficial EPA and deep EPA both come from the SFA. This type of origin of the EPA was noted in 5 cases. Depending on the side, it was observed twice on the right and three times on the left; by sex, it was observed 4 times in men and 1 time in women.
The fourth type of origin was the origin of the superficial EPA of the quadricipital artery and the deep EPA of the SFA (Fig. 5). This type of origin has been observed in a man on the right.
In the 2 cases where there were 3 EPA, the superficial EPA came from the CFA and the meddle and deep EPA came from by a common trunk of the SFA. One of these 2 cases was observed in a man on the right; the other case was observed in a woman on the left.
Original mode
In all cases where there was only one EPA, it was born in isolation (Figs. 2 and 3). Among the cases where there were 2 EPA, in 15 cases (20, 83) the superficial EPA and the deep EPA originated in isolation (Fig. 4). This mode of birth was observed 7 times on the right and 8 times on the left. According to sex, it has been observed 13 times in men 2 times in women. In 13 cases (18.06%), the superficial EPA and the deep EPA originated through a common trunk (Fig. 6). Depending on the side, this mode of birth was observed 4 times on the right and 9 times on the left. By sex, it has been observed 9 times in men and 4 times in women. In 2 cases, the superficial EPA originated through a common trunk with the superficial epigastric artery, and the deep EPA originated in isolation. These 2 cases were observed in men on the right.
Among the 2 cases where there were 3 EPA, in 1 case the superficial EPA originated by a common trunk with the superficial epigastric and iliac circumflex arteries; the middle and deep EPA originated by a common trunk. This disposition was noted in a man on the right. In the other case, the superficial EPA originated by a common trunk with the inferior epigastric artery; the middle and deep EPA were born by a common trunk. This disposition was observed in a woman on the left.
Reports of the external pudendal artery with the arch of the great saphenous vein
The most frequent relationship of the EPA with the arch of the GSV was the sub-crossing of the arch of the GSV by the single EPA (Fig. 3). This disposition was observed in 32 cases (44.44%). Depending on the side, it was observed in 17 cases on the right and in 15 cases on the left; by sex, it was observed in 25 cases in men and in 7 cases in women.
In 7 cases (9.72%), there was a single EPA which pre-crossed the GSV passing behind the lateral accessory saphenous vein (Fig. 2). According to the side, this report was noted 4 times on the right and 3 times on the left; by sex, it was noted only in men.
In 11 cases (15.28%), the superficial EPA and the deep EPA originated in isolation, which the superficial EPA passing above the arch of the GSV, and the deep EPA passing below of the arch of the GVS (Fig. 4). Depending on the side, this arrangement was observed 5 times on the right and 6 times on the left; by sex, it was observed 9 times in men and 2 times in women.
In 6 cases (8.33%), the superficial EPA and the deep EPA originated by a common trunk that divided before reaching the arch of the GVS, then the superficial EPA passed over the arch of the GSV and the deep EPA passed below the arch of GVS. Depending on the side, this layout was noted twice right and 4 times left; by sex, it was noted 5 times in men and 1 time in women.
In 5 cases (6.94%), the two EPA (superficial and deep) originated in isolation and both passed below the arch of the GSV. This disposition was observed only in men, 3 times on the right and 2 times on the left.
In 3 cases, a common trunk passed below the arch of the GSV before dividing into superficial EPA and deep EPA. One of these 3 cases was observed on the right and the other 2 cases were observed on the left. According to sex, this disposition was observed 1 time in men and 2 times in women.
In 2 cases, the trunk common to both superficial and deep EPA passed behind the lateral accessory saphenous vein before dividing in front of the GSV. These 2 cases were observed in men, once on the right and on the left.
In 1 case, the common trunk of the two superficial and deep EPA divided before reaching the arch of the GSV, and the two superficial and deep EPA crossed the GSV by passing behind the lateral accessory saphenous vein (Fig. 6). This case was observed in a woman on the left side.
In 1 case, the superficial EPA and the deep EPA originated separately and both pre-crossed the GSV (Fig. 5). This case was observed in a man on the right.
In 1 case, the common trunk of the superficial and deep EPA divided before reaching the arch of the GSV, the superficial EPA pre-crossed the GSV passing behind the lateral accessory saphenous vein, and the deep EPA has passed behind from the GSV. This case was observed in a man on the left.
In 1 case, the GSV was duplicated and the single EPA passed between the 2 trunks. It passed behind the lateral trunk and in front of the medial trunk. This case was observed in a man on the right.
In the 2 cases where there were 3 EPA, the superficial passed over the arch of the GSV, the middle and the deep crossed the arch of the GSV after the division of their common trunk. One of these 2 cases was observed in a man on the right and the other case was observed in a woman on the left.
DISCUSSION
Number
In the present study, the EPA was visible in all cases. According to Hemmati et al. (2012), in their study of 228 patients who underwent surgery, the EPA was identified during all surgical explorations. Manerikar et al. (2015), in their study of 50 patients who underwent Trendelenburg surgery with GVS stripping, noted that the EPA was not seen in 2 patients (4%). According to Ramalingam and Rajeswari (2018), in a series of 50 cases, superficial EPA was not identified in 8 cases (16%). According to Preethiramya (2008), in 37 out of 50 cases (74%), the EPA was not seen at the saphenofemoral junction. According to Souroullas et al. (2016), in their study on the anatomy of the saphenofemoral junction in a consecutive series of 172 patients undergoing ligation of the unilateral primary saphenofemoral junction, EPA was identified in 150 cases (87.2%). La Falce et al. (2006), in their study, found the EPA in 46 out of 50 cases (92%).
In this study, the presence of a single EPA was the most common. It was noted in 40 cases (55.56%). Castro et al. (1998) found in their study that the EPA was a single vessel in 55% of the cases. Henriet (1987) shows that, among 256 patients, 80% of women and 65% of men have a single APE. According to Gaye et al (2016), out of 22 dissected inguinal regions, in 15 cases (68.18%), there was only one EPA. In all of these studies, the presence of a single EPA was the most common, which confirms our results.
The presence of two EPA as noted in the anatomical works occupied the second position in this study. 30 cases (41.67%) were observed with a non-significant difference, since P>0.05. Gaye et al (2016) also found it in second position, with 6 cases out of 22 with male predominance and on the right side. Henriet (1987) also finds this second position, but with a predominance of men and on the right side. According to Castro et al. (1998), the EPA was double in 30%, and with a common core in 15%.
The existence of three pudendal arteries is exceptionally reported in the literature (Gaye et al., 2016). In the present study, the presence of three APE was noted in 2 cases. Gaye et al. (2016) found, in their series, a common arterial trunk that trifurcates into three arterial branches, which they have named upper, middle and lower external pudendal arteries. This same observation is made by Henriet (1987) who, in addition, pointed out another rare provision namely three external pudendal arteries originating in isolation from the common femoral artery.
Origin
In the present study, in cases where there was only one EPA, it came from the CFA in 18 cases and from the SFA in 22 cases. Of the cases where there were two superficial and deep EPA, they were both from the CFA in 17 cases; in 7 cases, the superficial EPA came from the CFA and the deep EPA from the SFA; in 5 cases, the superficial EPA and deep APE both came from the SFA; in 1 case, the superficial APE came from the quadricipital artery and the deep APE from the SFA. Gaye et al. (2016) noted that, in their series, all the external pudendal arteries originate from the common femoral artery. Falce (2006) confirms this exclusive origin on the common femoral artery, from a series of dissection of 50 inguino-femoral regions on anatomical subjects. An origin at the level of the deep femoral artery is described by 3 authors. Donnelly (2005) shows, out of a series of 2080 dissected inguinal regions, that 4.6% of external pudendal arteries have an origin on the deep femoral artery. Castro et al. (1998) noted in 1 in 20 dissections that the EPA originated from the deep femoral artery. In addition, Tanyeli (2006) describes this same origin on an isolated case of dissection. The origin of the APE of the superficial femoral artery was noted in 19 cases during a study of 20 dissections by Castro et al. (1998). Apart from this last study and ours, this origin of the APE has not been noted in English and French literature. In contrast, a superficial APE from the quadricipital artery as in this study has not been reported in the English and French literature.
Variations in the branching pattern of the femoral artery can be explained on the basis of abnormal development of the arterial network of the pelvic limb of the embryo (Çiftcioglu et al., 2009). The axial artery of the pelvic limb is derived from the fifth lumbar intersegmental artery. It is considered to be the branch of the internal iliac artery and extends over the face of the thigh. The femoral artery runs along the ventral surface of the thigh, opening a new canal to the pelvic limb. It arises from a capillary plexus that is connected proximally with the branches of the external iliac artery and distally with the axial artery (Standring et al., 2008). It is believed that the increased blood flow in these capillaries determines the final mature arterial pattern. Thus, the most suitable channels enlarge while others contract and disappear (Çiftcioglu et al., 2009; Prakash Kumari et al., 2010). Thus, the original variations of the EPA could be explained by the situation of the blood vessels going to the external genitalia in which the blood flow is increased.
Original mode
In the present study, in all cases where there was only one EPA, it originated in isolation. The existence of two EPA (superficial and deep) that are born separately was noted in the present study in 15 cases (20.83%). Gaye et al. (2016) found it in two patients. Henriet (1987) noted it in 15 out of 149 patients. On the other hand, La Falce (2006) noticed it a little more frequently, with 21 cases out of 46 external pudendal arteries found. The existence of two APE (superficial and deep) that arise through a common trunk was observed here in 13 cases (18.06%). La Falce (2006) found this configuration in 24% of his dissections. It was found in 25% of cases by Peera and Sugavasi (2013). The existence of two EPA, the superficial EPA of which originates through a common trunk with the inferior epigastric artery while the deep EPA is born separately, was observed in the present study in 2 cases. According to Nafees and Usmani (2018), in 2 cases out of 25 dissected lower limbs, the superficial EPA appeared as a common trunk with a superficial epigastric artery. This same configuration was noted by Myageri et al. (2018) in 5 out of 40 cases (12%), and by Taylor and Daniel (1975) in 3 out of 20 cases (15%). The existence of three APEs, of which the superficial EPA originates from a trunk with the superficial epigastric arteries and superficial iliac circumflex, or with the inferior epigastric artery, while the middle and deep PAE arise from a common trunk reported in the literature. Gaye et al. (2016) noted in 1 case an arterial trunk, which is divided into three upper, middle and lower EPA. The exceptional arrangement illustrated by three upper, middle and lower external pudendal arteries, which have separate origins on the common femoral artery, has been described in one patient by a single author (Henriet, 1987).
Reports of the external pudendal artery with the arch of the great saphenous vein
o In the present study, the most frequent report was the sub crossing of the arch of GSV by the single EPA. The latter passed behind the GSV and in front of the femoral vein. We noted it in 32 cases (44.44%). Gaye et al. (2016) found that the single EPA crosses the butt of the GSV in 8 out of 22 cases. This provision was noted by Henriet (1987) in 70.4% of the cases. According to Ramalengam and Rajeswari (2018), in their series of 50 dissections, in 26 cases (52%), the superficial EPA was found posterior to the great saphenous vein. Ruji (2016) in 72 of 80 cases, or 90% of the cases in his study, was able to clearly demonstrate the superficial EPA between the GSV and the common femoral vein. Hemmathi et al. (2012) studied 228 varicose vein patients who underwent surgery. They noted that the EPA crossed behind the saphenofemoral junction in 60.5%. Manerikar et al. (2015) studied 50 patients who underwent Trendelenburg surgery with stripping of a large saphenous vein. They found that the superficial EPA crossed the saphenofemoral junction posteriorly in 28 (56%) patients. These different studies and ours have noted that the passage of the EPA below the arch of the GSV and behind the GSV is the most frequent report. Ndiaye (2006) finds, in his series, 50% of external pudendal arteries that under-intersect the arch of the great saphenous vein. This report exposes to lesions of the external pudendal artery, during the dissection of the proximal part of the trunk of the great saphenous vein. We can also confuse, at the time of ligation of the venous afferents of the arch of the great saphenous vein, the terminal part of the external pudendal artery and the external satellite pudendal vein (Gaye et al., 2016).
The existence of the two isolated EPA, whose superficial EPA passes over the arch of the GSV, and the deep EPA crosses the butt of the GSV, was the second most frequent report in the present study. This is the classic relationship of EPA with the arch of GSV noted in the anatomy books. We noted it in 11 cases (15.28%). This provision noted in 1 case by Gaye et al. (2016), in 8 cases out of 10 (80%) by Mostafa (2006).
In the present study, in 7 cases (9.72%), there was a single APE that pre-crossed the GSV passing behind the lateral accessory saphenous vein. Donnelly et al. (2005) describe an external pudendal artery which passes between a great saphenous vein and an accessory saphenous vein in 4.6% of his observations. Henriet (1987) describes an external pudendal artery that passes between the great saphenous vein and the vein of Jacomini. These situations increase the surgical difficulty, and at the same time the risk of injury to the external pudendal artery (Gaye et al., 2016).
In the present study, in 6 cases (8.33%), the superficial EPA and the deep EPA originated by a common trunk that divided before reaching the arch of the GSV, including the superficial EPA, which passed over the arch of the GSV, and the deep EPA, which passed below the arch of the GSV. This provision was noted by Mostafa (2006) in 1 case.
The existence of two isolated EPA (superficial and deep) that both passed below the arch of the GSV was observed in 5 cases (6.94%) in the present study. Gaye et al. (2016) noted this provision in 1 case.
A common trunk of the two EPA (superficial and deep) which passes below the arch of the GSV before dividing was observed 3 times in the present study. Mostafa (2006), in his study, noted that in 1 case there was a single long external pudendal trunk that followed the same course of the deep external pudendal artery. It gave branches similar to the superficial external and deep external arteries.
In the present study, in 1 case, the common trunk of the superficial and deep EPA divided before reaching the arch of the GSV, the superficial EPA pre-crossed the GSV by passing behind the accessory lateral saphenous vein, and the deep EPA passed behind the GSV. Gaye et al. (2016) noted, in 1 case, the single trunk which, before reaching the arch, divides and surrounds it like forceps. This latter arrangement is described once by Ndiaye (2006).
In the present study, in 1 case, the GSV was duplicated and the single EPA passed between the 2 trunks. It passed behind the lateral trunk and in front of the medial trunk. According to Donnelly et al. (2005), in 4.6%, the EPA passed back to a large tributary or a trunk of the bifid GSV and in front of the second trunk, making identification of the second trunk particularly difficult. This last finding is similar to our case. Gaye et al. (2016) had found, in one patient, a GSV presenting a single trunk with a double stick throwing itself on the common femoral vein, and passage of a single EPA in this loop formed by the two sticks and the trunk of the GSV.
CONCLUSION
Most often, there is only one EPA. When there are two EPA, they can originate in isolation or through a common core. The EPA contracts variable and close relationships with the arch of the GSV. Since lesions of the EPA can lead to impotence, these reports must be known by surgeons to avoid damaging the EPA during surgical treatment of varicose veins of the pelvic limb.
ACKNOWLEDGEMENTS
We thank Pr Mohamed Keïta for correcting the article and for his encouragement, Dr Mahamoud Cissé for doing statistical test of the article, and Pr Seydou Doumbia for his financial support to the Bamako anatomy laboratory.