The aim of this study is to describe the morphology and prevalence of anatomical variants of the celiac trunk (CT) inMexican population, a crucial vascular structure while planning interventional radiology or surgery of the abdominalregion. 127 Multidetector-row CT angiographies (MDCTA) from patients in the National Institute of Medical Sciencesand Nutrition “Salvador Zubirán” (Mexico) were analyzed. Sixty-seven were women and sixty were men, with age rangebetween 20 and 74 years old and with not previous pathologies reported. Ethics committee approval was obtained for thisstudy. Anatomical variants were classified according to Marco-Clement’s classification (2016). Type I, Complete CT, wasfound in 109 patients (109/127; 85.8%). The mean length of the CT was 20.4 mm ± 6.5 mm (range: 6.1-44 mm). Ostiummean diameter was 7.7 mm ± 1.9 (range 4.1-18.9 mm). Mean distance between the CT and the superior mesenteric arterywas 7.3 mm ± 3.5 mm (range: 0.7-17.2 mm). Type II, incomplete CT, was found in 17 patients (17/127; 13.4%): subtypeIIa, hepato-splenic trunk, was found in 9 patients (9/127; 7.1%), and subtype IIb, gastro-splenic trunk, in 8 patients(8/127; 6.3%). We did not observe Type III, independent origin of all arteries of the trunk or absence of CT. Type IV,celiac-mesenteric trunk, was found in 1 patient (1/127, 0.8%). No significant differences between genders were observed. This is the first study in Mexican population that describes CT variants by MDCTA using the newest classification withclinical significance prior to surgery or radiologic intervention.
Variations of the celiac trunk in Mexican population by MDCT angiography
Rodrigo A. Estrada León1, Gustavo Barraza Aguirre2, Vicente Toledo Coronado2, Dulce A. Sánchez Nava2, Monica Chapa Ibargüengoitia2, Mariana Díaz Zamudio2, Jorge Alanis Mendizabal1, José J. Martínez De Anda1, Diego Pineda-Martinez1
1 Department of Innovation in Human Biological Material, Faculty of Medicine, National Autonomous University of Mexico
2 Department of Radiology and Image, National Institute of Medical Sciences and Nutrition "Salvador Zubirán" CDMX, Mexico
SUMMARY
Sign up or Login
INTRODUCTION
Assessment of the upper abdominal circulation is crucial while planning interventions involving the liver, bile duct, stomach, pancreas and spleen. Awareness of the anatomical variants improves outcomes in radiologic diagnosis, interventions and surgery by decreasing the rate of complications and morbidity (Ugurel et al., 2010; Nghiem et al., 1999; Clark, 2006; Winston et al., 2007; Osman and Abdrabou, 2016).
The celiac trunk morphology was described in 1756 by Albrecht von Haller, a Swiss anatomist and physiologist (Haller, 1756; Venara et al., 2013; Osman and Abdrabou, 2016). The classic pattern or complete trunk is made up by the left gastric artery (LGA), the splenic artery (SA) and the common hepatic artery (CHA) (Vandamme and Bonte, 1985). The superior mesenteric artery (SMA), which irrigates the pancreas, small intestine, cecum, ascending colon and the proximal transverse colon, has been reported also taking part in the celiac trunk as a fourth branch or celiac-mesenteric trunk (Sehgal et al., 2013).
The morphology and variations of the CT have been reported since the late nineteenth century. Furthermore, as usual in anatomical studies, no single universal classification has been proposed, resulting in a wide range of classifications (Lipshutz, 1917; Adachi, 1928; Michels, 1955; Song et al., 2010; Panagouli et al., 2013). There is only one study that made a meta-analysis of this variations using previous classifications proposals (Marco-Clement et al., 2016), and there is a research study made by our group based on pathological dissections analyzing TC variations in Mexican population (Pineda et al., 2019). Therefore, we have undertaken this study with the aim of using a simpler and unified classification of the celiac trunk’s variations in patients.
MATERIALS AND METHODS
This retrospective study was approved by the institutional review board. Informed consent requirement was waived.
Patient population
The study was performed analyzing the MDCT scans from 200 consecutive patients from the radiological archive of the National Institute of Medical Sciences and Nutrition “Salvador Zubirán” in Mexico City between January and March of 2017.
Patients with tomographic studies that included an early arterial angiographic phase were included. The indication for such studies were: preoperative evaluations or follow-up for pancreatic or hepatobiliary neoplasms, kidney donation protocols, and monitoring of hyper-vascular gastrointestinal neoplasms. Patients with history of surgery, neoplasia, or atheroma plaques involving the celiac trunk or their branches were excluded.
Technical Parameters
The tomographic images were obtained using two 64-detector helical tomography equipments. The Somatom Sensation 64 equipment (Siemens, Germany) with the following technical parameters: 120 kV, 220 mAs, 64 x 0.6 mm acquisition, 0.5 sec rotation time, 0.95 pitch reconstruction at 3 mm, and the LightSpeed VCT equipment (General Electric Medical Systems, Milwaukee, Wisconsin, USA) with parameters 120 kV, 700 mAs, acquisition 40 x 2.5 mm, rotation time of 0.5 sec. 1,375 pitch, 3 mm reconstruction. 80-100 ml of intravenous non-ionic contrast medium (Iopromide, Ultravist 370; Schering, Berlin, Germany) were used at an infusion rate of 3 - 4 ml / sec followed by a 40 ml bolus of saline, using an automatic injector.
The injection was performed through a 16-18G forearm route or through a jugular central venous catheter in hospitalized patients. Arterial acquisition was performed at 35 seconds with a craniocaudal scan in apnea after deep inspiration. Most of the arterial tomographic series evaluated were part of multiphasic protocols with subsequent acquisitions in portal phases (40-60 sec), venous (80 sec) or late (3 min).
Image analysis
Three radiologists in training: (G.B., V.I.T.C., D.A.S.N.) with 4, 3 and 3 years of experience in abdominal imaging, respectively, jointly reviewed all the MDCTAs and the angiographic images on a picture archiving and communication systems (PACS) workstation (Carestream Vue, version 12.1.5, Carestream Health, Rochester, NY, USA).
CT variants were registered on a database using the Microsoft Excel calculation program (Microsoft Corporation, USA), and the data analysis was performed with the Stata statistical program (StataCorp, USA). To perform the different measurements, multiplanar reconstructions and the linear or curved measurement tools were used in the Picture Archiving and communications system “PACS” (Carestream, Rochester, NY, USA).
Three-dimensional volumetric reconstructions and maximum intensity projections were obtained to demonstrate the most representative variants. The morphology of CT was classified according to Marco-Clement (Marco et al., 2016).
Statistical analysis
Data are presented as number and relative percentages. Quantitative variables are expressed as mean value. We compared categorical variables with the Fisher or the Chi-square test, as appropriate. For continuous variables, we used Student’s t-test for parametric data distribution. P- value < 0.05 was considered statistically significant.
RESULTS
Patients
During this research, MDCT angiographies from 200 patients were analyzed, of which 73 were excluded due to surgical history, neoplasia or atheroma plaques involving the celiac trunk or branches. In total 127 patients were included for the main analysis, 67 (52.8%) female and 60 (47.2%) male. The mean age was 49.3 ± 14.1 years (range: 20-85 years).
CT Classification
We describe variations according to the previously commented classification that use four main types of CT (Marco-Clement et al., 2016). Distribution according Type and Gender is shown in Table 1.
Type I
Complete trunk in which LGA, SA and CHA arise from a common trunk was found in 109 patients (109/127; 85.8%) (Fig. 1). As Type I is considered to be a proper celiac trunk, morphometric values were analyzed only in this group. We measured the CT length, ostium diameter and distance between the CT and the superior mesenteric artery. The mean length of the CT was 20.4 mm ± 6.5 mm (range: 6.1-44 mm). Ostium mean diameter was 7.7 mm ± 1.9 (range 4.1-18.9 mm). Mean distance between the CT and the Superior mesenteric artery was 7.3 mm ± 3.5 mm (range: 0.7-17.2 mm) (Table 2).
In Type Ia, LGA arise from the CT prior to the origin of CHA and SA. It was observed in 81 patients (81/127; 63.8 %). Type Ib corresponds to the classical Haller’s Tripod, a trifurcated entity with an equidistant origin of LGA, SA and CHA. It was observed in 27 of patients (27/127; 21.3%). Type Ic is a trunk with an additional arterial branch (accessory common hepatic, dorsal pancreatic, phrenic or gastroduodenal). This pattern was observed in 1 patient (1/127; 0.8%).
Type II
Incomplete trunk in which either LGA, CHA and SA do not participate in the CT was found in 17 patients (17/127; 13.4 %). Gender distribution is shown in Table 1.
Type II is divided into three subtypes:
Type IIa, hepato-splenic trunk was detected in 9 patients (9/127;7.1 %) (Fig. 2).
Type IIb, gastro-splenic trunk was reported in 8 patients (8/127; 6.3%) (Fig. 3).
Type IIc, hepato-gastric trunk, was not found in our patients.
Type III, absence of the celiac trunk was not found in our patients (0%).
Type IV
Celiac-mesenteric trunk was found in 1 female (1/127; 0.8%) (Fig. 4).
Statistical analysis using Chi square test (a = 0.05) revealed no significant differences between genders in the presence of a CT variants, types or subtypes between genders.
DISCUSSION
MDCT angiography has become the primary tool for the evaluation of patients with suspected abnormalities of abdominal vessels. Three-dimensional and multiplanar imaging are non-invasive ways to examine the morphology of the celiac trunk and its branches, playing an important role by providing proper description and roadmaps of arterial morphology, previous surgical and radiological procedures such as liver transplantation or arterial chemoembolization (Nghiem et al., 1999; Winston et al., 2007; Song et al., 2010). This image techniques reduce morbidity and mortality in pathologies as median arcuate ligament syndrome, celiac trunk aneurysm, celiac artery stenosis and occlusion. They are also used for detecting early vascular complications in post-intervention surveillance (Hiatt et al., 1994; Clark, 2006; Osman and Abdrabou, 2016).
The morphology of the abdominal vascular anatomy is highly variable and the celiac trunk (CT) is not an exception to this fact (Lippert Hans, 1985). Michels (1955) reported variation of the CT in 11% of its cadaver dissections. Similar rates have been reported on cadaveric studies with a range from 26.6 %, 15.7% (Lipshutz, 1917; Winter et al., 1995). In the MDCT era, Song et al. (2010) reported variations in 10.9% of their patients. Several image studies have reported prevalence of: 27.9%, 14.1 % and 9.5 (Eaton, 1917; Vandamme and Bonte, 1985; Hazirolan et al., 2009; Johnson et al., 2013; Marco-Clement et al., 2016). We found CT variations in 18 patients (18/127; 14.2%). In contrast, a previous cadaveric study in Mexican population reported a variation rate of 6% (Pineda et al., 2019).
Although using MDCT-angiography we obtained a higher prevalence of CT variation (14.2%), there was no statistically significant difference (p>0.05) with the prevalence of CT variations (6%) obtained in the first Mexican dissection study (Pineda et al., 2019).
Previous researches made by cadaver dissection and MDCT angio-tomography have described and published different classification systems according with their particular. Lipshutz (1917) described four CT patterns; Eaton (1917) proposed four geometrical categories; Adachi (1928) and Michels (1955) described six main groups based on cadaveric dissection, and Song et al. (2010) divided CT morphology in three categories. A recent study made a compilation of published cadaveric and radiological series, unifying and proposing a simpler and useful classification of 4 main Types (Marco-Clement et al., 2016). In Table 3 we describe the results and discussion according to this new and universal classification.
Type I
Type I (complete trunk), in which LGA, SA and CHA arise from a common trunk, was the most frequent Type reported in researches among general population with an observed prevalence of 72.1% to 90.5% (Iezzi et al., 2008; Marco-Clement et al., 2016). It was present in 109 of our patients (109/127; 85.8%). We agree with previous studies in the statement that Type I is the most common pattern observed. As Type I is considered to be a proper celiac trunk, morphometric values were analyzed only in this group (see Table 2).
Type II
Type II (incomplete trunk) can be divided in three subtypes, type IIa, IIb and IIIc. This pattern was observed in 17 patients (17/127; 13.4 %). Previous studies have reported a Type II prevalence of 7.5%, 10.9 and 11% (Rossi, 1904; Uflacker, 2007; Song et al., 2010). As an incomplete pattern, this can be considered the most frequent morphology variation CT can acquire. Although not all the studies can be adjusted to the new classification criteria due to insufficient anatomy description, the ones that could be adapted were included in the following Subtypes II analysis.
For Subtypes II the following analysis was made.
Type IIa (hepato-splenic trunk), with independent emergence of the LGA, was the most frequent CT variation described in 9 patients (9/127; 7.1 %). It was also the most frequent type in studies made around in other countries such as Spain 4.45% (Marco-Clement et al., 2016), South Korea 4.42% (Song et al., 2010), Greece 3.34% (Panagouli et al., 2013) and Egypt 3% (Osman and Abdrabou, 2016).
Type IIb (gastro-splenic trunk), with independent emergence of CHA, was found in 8 patients (8/127; 6.3 %). The presence of this variation has been reported in range of between 0.22% and 5% in several studies (Winston et al., 2007; Song et al., 2010; Marco-Clement et al., 2016; Osman and Abdrabou, 2016). Although Michels (1955) and Eaton (1917) reported it as the most frequent variant present in 5.5% and 4.9% of their patients, it was the second most frequent variant reported in our study (distribution is shown in Table 3).
Type III
Type III (absence of celiac trunk) was not found in our sample. It has the lowest incidence reported: as with our research team, some other groups could not find it (Chen et al., 2009; Song et al., 2010; Marco-Clement et al., 2016). Other groups have reported its presence from 0.6% to 2% (Morita, 1935; Iezzi et al., 2008).
Type IV
Type IV (celiac-mesenteric trunk), the rarest variation form that the celiac trunk can acquire, interpreted as the result of the persistence of the large primitive ventral anastomosis between the early segmental celiac trunk and superior mesenteric groups (Tandler, 1904), was observed in only 1 female patient (1/127; 0.8%). This rare variation has been identified from 0.4% to 2.4% (Rossi, 1904; Lipshutz, 1917; Iezzi et al., 2008; Song et al., 2010; Osman and Abdrabou, 2016).
Statistical analysis using Chi square test (a = 0.05) revealed no significant differences in the presence of CT variants, types or subtypes between genders. Several studies have confirmed this lack of relation between gender and the presence of CT variation, although a relation with ethnicity has been shown (Panagouli et al., 2013). More studies should be made to assure it.
Related articles


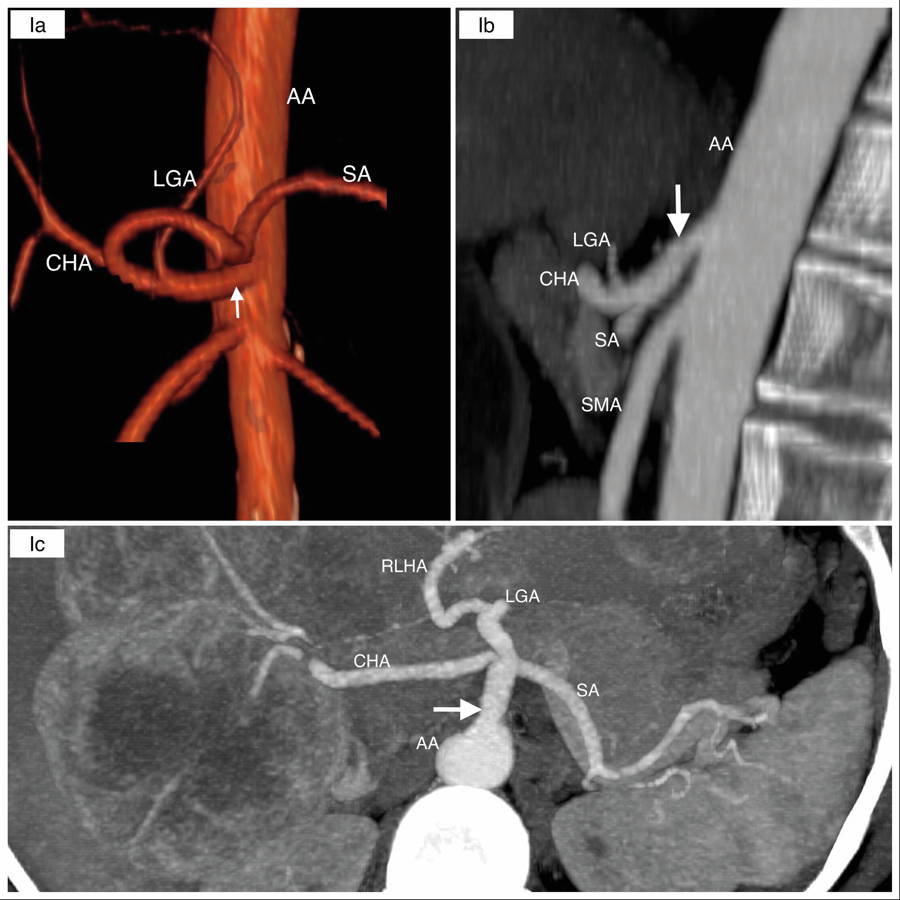 Fig. 1.- Type I” Complete Trunk: Ia: Complete bifurcated celiac trunk (LGA arises first); Ib: Complete trifurcated celiac trunk and Ic: Complete celiac trunk with extra branch. Abdominal Aorta (AA), Left Gastric Artery (LGA), Common Hepatic Artery (CHA), Splenic Artery (SA), Replaced Left Hepatic Artery (RLHA), White arrow (Celiac Trunk). In max intensity projection of sagittal reconstruction (first image) In three dimensional volumetric reconstruction (Ia) and Max intensity projection of sagittal reconstruction (Ib & Ic).
Fig. 1.- Type I” Complete Trunk: Ia: Complete bifurcated celiac trunk (LGA arises first); Ib: Complete trifurcated celiac trunk and Ic: Complete celiac trunk with extra branch. Abdominal Aorta (AA), Left Gastric Artery (LGA), Common Hepatic Artery (CHA), Splenic Artery (SA), Replaced Left Hepatic Artery (RLHA), White arrow (Celiac Trunk). In max intensity projection of sagittal reconstruction (first image) In three dimensional volumetric reconstruction (Ia) and Max intensity projection of sagittal reconstruction (Ib & Ic).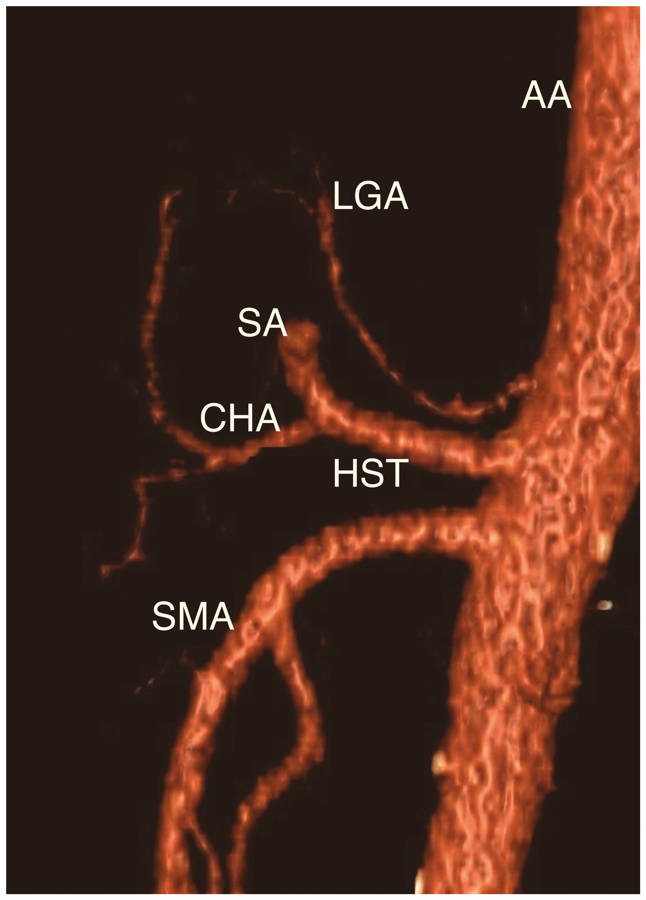 Fig. 2.- Three-dimensional volumetric reconstruction. “Type IIa” Hepatosplenic trunk (HST) with Left Gastric Artery (LGA) arising from the Abdominal Aorta (AA). Common hepatic Artery (CHA), Splenic Artery (SA) and Superior Mesenteric Artery (SMA) were identified.
Fig. 2.- Three-dimensional volumetric reconstruction. “Type IIa” Hepatosplenic trunk (HST) with Left Gastric Artery (LGA) arising from the Abdominal Aorta (AA). Common hepatic Artery (CHA), Splenic Artery (SA) and Superior Mesenteric Artery (SMA) were identified.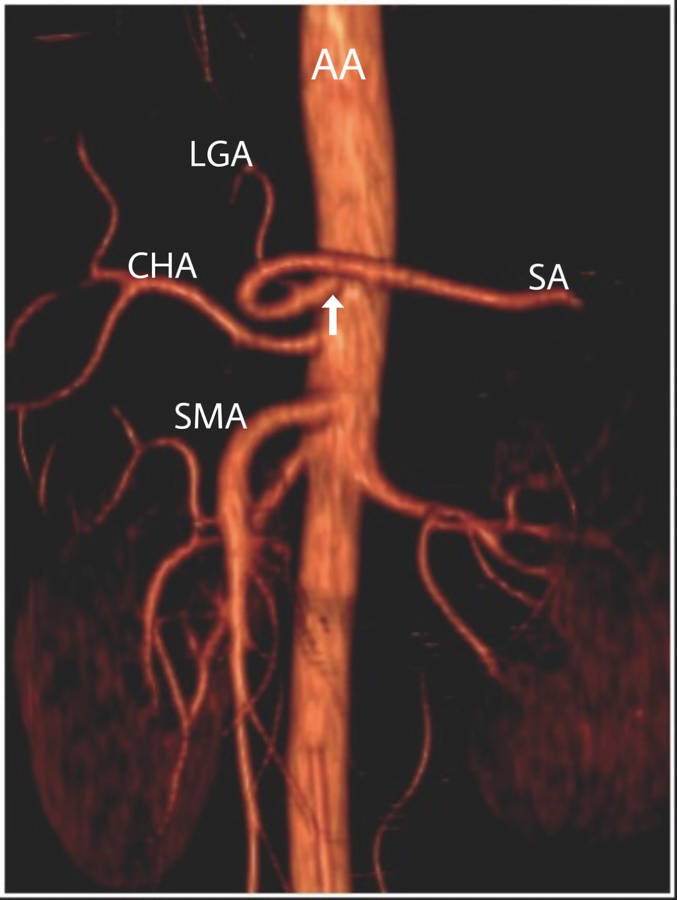 Fig. 3.- Three-dimensional volumetric reconstruction. “Type IIb” Gastrosplenic trunk (white arrow), Common Hepatic Artery (CHA) arising from the Abdominal Aorta (AA). Left Gastric Artery (LGA), Splenic Artery (SA) and Superior Mesenteric Artery (SMA) are shown.
Fig. 3.- Three-dimensional volumetric reconstruction. “Type IIb” Gastrosplenic trunk (white arrow), Common Hepatic Artery (CHA) arising from the Abdominal Aorta (AA). Left Gastric Artery (LGA), Splenic Artery (SA) and Superior Mesenteric Artery (SMA) are shown. 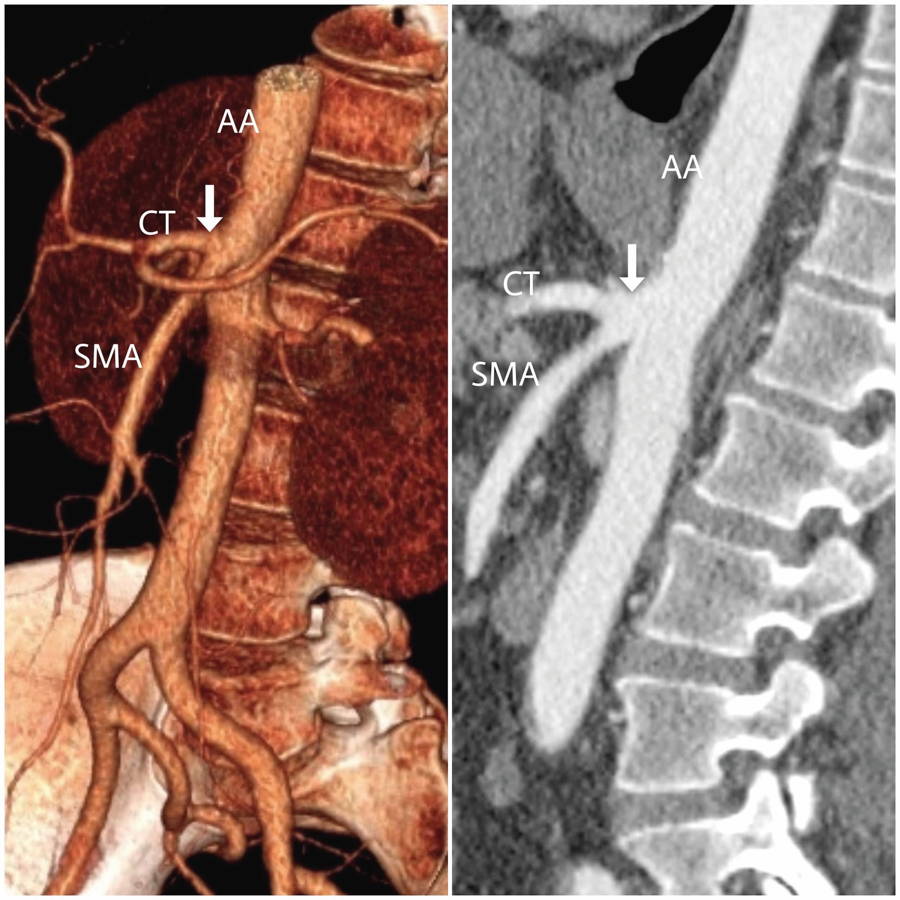 Fig. 4.- “Type IV” Celiac Trunk (CT) and Superior Mesenteric Artery (SMA) arising together from the Abdominal Aorta (AA) in a Celiac mesenteric Trunk (white arrow). Three-dimensional volumetric reconstruction (left image) and max intensity projection of sagittal reconstruction (right image).
Fig. 4.- “Type IV” Celiac Trunk (CT) and Superior Mesenteric Artery (SMA) arising together from the Abdominal Aorta (AA) in a Celiac mesenteric Trunk (white arrow). Three-dimensional volumetric reconstruction (left image) and max intensity projection of sagittal reconstruction (right image).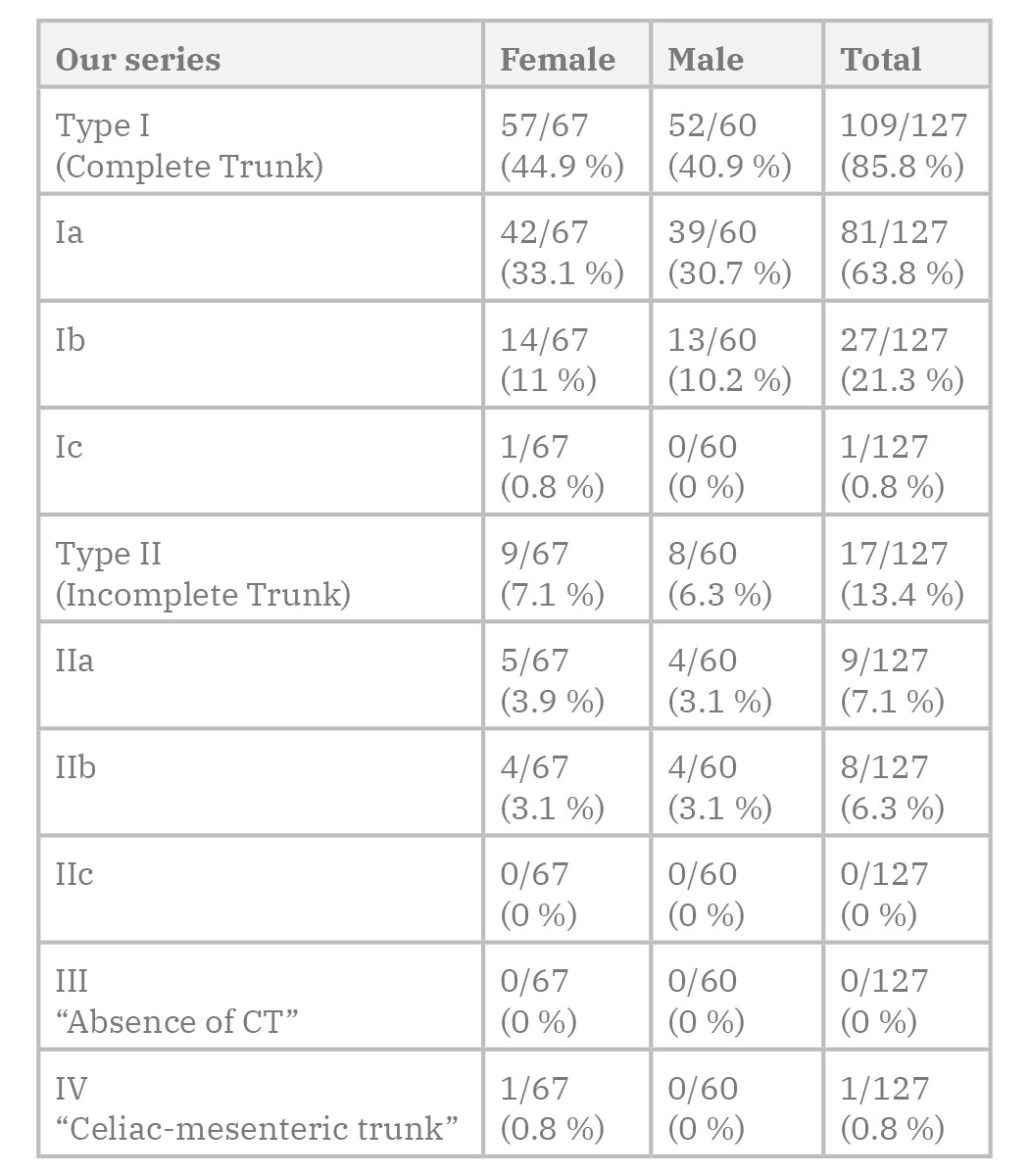 Table 1. Incidence of variations of the celiac trunk by gender in our MDCT-angiography research.
Table 1. Incidence of variations of the celiac trunk by gender in our MDCT-angiography research.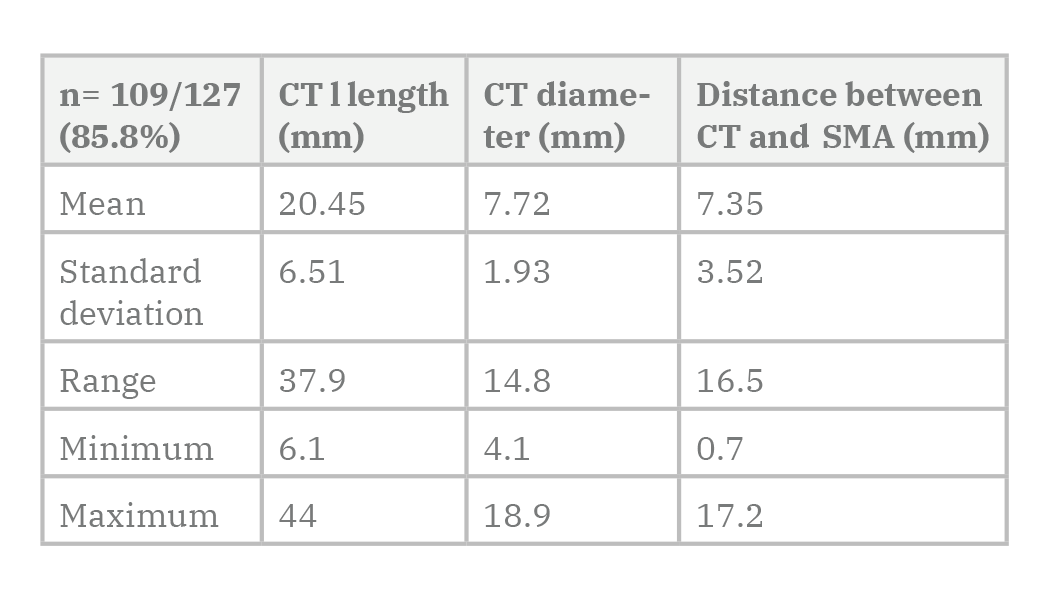 Table 2. Morphometric values of the Celiac Trunk (CT) Type I (complete Trunk).
Table 2. Morphometric values of the Celiac Trunk (CT) Type I (complete Trunk).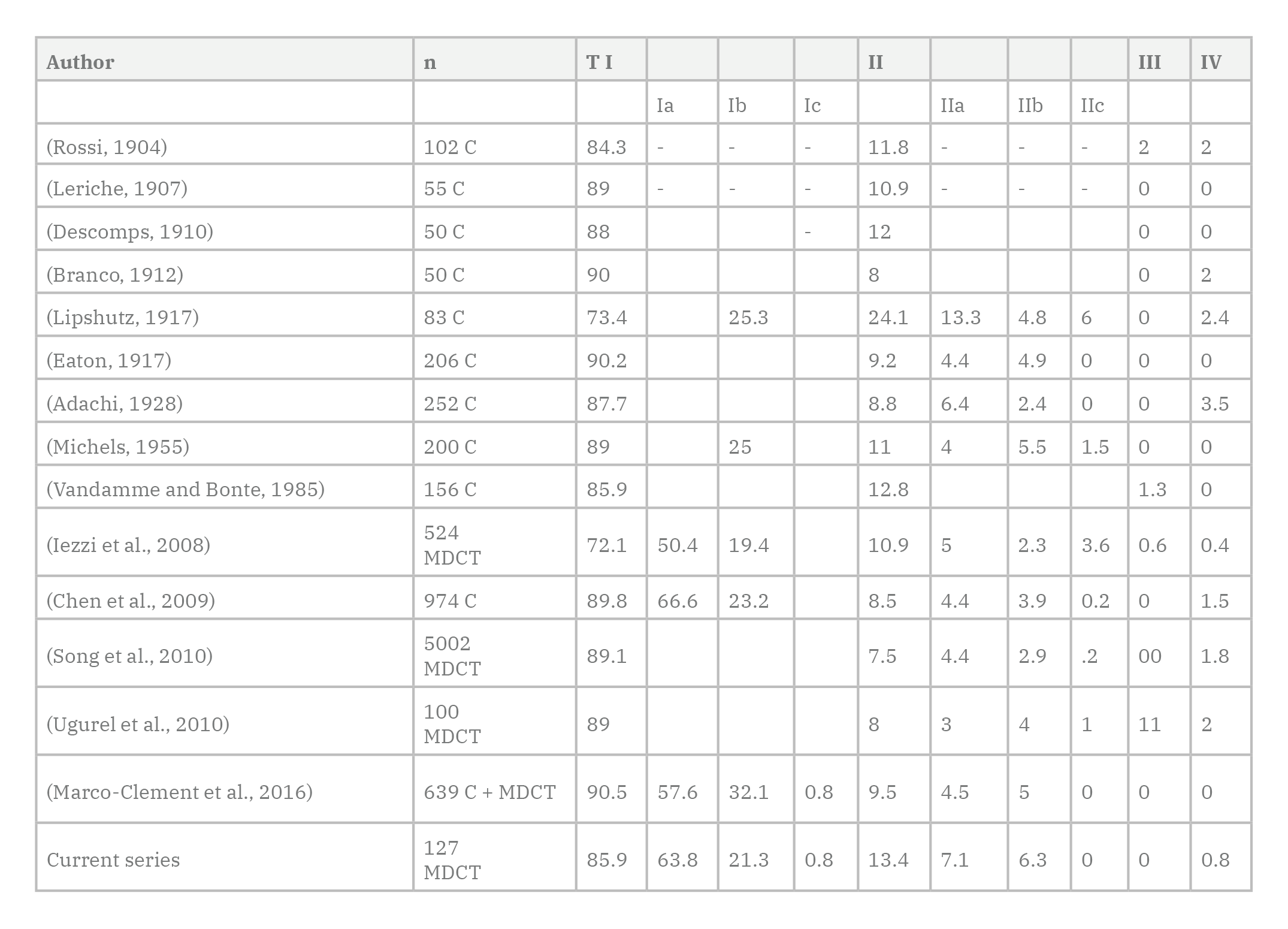
ADACHI B (1928) Das Arteriensystem der Japaner. Vol II. Maruzen Publishing Co, Kyoto.
CHEN H, YANO R, EMURA S, SHOUMURA S (2009) Anatomic variation of the celiac trunk with special reference to hepatic artery patterns. Ann Anat, 191: 399-407.
CLARK TWI (2006) Complications of hepatic chemoembolization. Semin Intervent Radiol, 23: 119-125.
EATON PB (1917) The coeliac axis. Anat Rec, 13: 369-374.
HAZIROLAN T, METIN Y, KARAOSMANOGLU AD, CANYIGIT M, TURKBEY B, OGUZ BS, ARIYUREK M (2009) Mesenteric arterial variations detected at MDCT angiography of abdominal aorta. Am J Roentgenol, 192: 1097-1102.
HIATT JR, GABBAY J, BUSUTTIL RW (1994) Surgical anatomy of the hepatic arteries in 1000 cases. Ann Surg, 220: 50-52.
IEZZI R, COTRONEO AR, GIANCRISTOFARO D, SANTORO M, STORTO ML (2008) Multidetector-row CT angiographic imaging of the celiac trunk: Anatomy and normal variants. Surg Radiol Anat, 30: 303-310.
JOHNSON PB, CAWICH SO, ROBERTS P, SHAH S, GARDNER MT, GORDON-STRACHAN G, PEARCE NW (2013) Variants of hepatic arterial supply in a Caribbean population: A computed tomography based study. Clin Radiol, 68: 823-827.
LERICHE FV (1907) Recherches anatomiques sur les artères de l’estomac. Bibliogr Anat, 16: 111.
LIPPERT HANS PR (1985) Arterial Variations in Man: Classification and Frequency. J.F. Bergmann Verlag, München, pp 30-47.
LIPSHUTZ B (1917) A composite study of the celiac axis artery. Ann Surg, 65: 159-169.
MARCO-CLEMENT I, MARTINEZ-BARCO A, AHUMADA N, SIMON C, VALDERRAMA JM, SANUDO J, ARRAZOLA J (2016) Anatomical variations of the celiac trunk: cadaveric and radiological study. Surg Radiol Anat, 38: 501-510.
MICHELS NA (1955) Blood supply and anatomy of the upper abdominal organs with a descriptive atlas. Lippincott Company, Philadelphia, pp 136-147.
MORITA M (1935) Reports and conception of three anomalous cases in the area of the celiac and superior mesenteric arteries [in Japanese]. Igaku Kenkyu, 9: 1993-2006.
NGHIEM HV, DIMAS CT, MCVICAR JP, PERKINS JD, LUNA JA, WINTER TC, HARRIS A, FREENY PC (1999) Impact of double helical CT and three-dimensional CT arteriography on surgical planning for hepatic transplantation. Abdom Imaging, 24: 278-284.
OSMAN AM, ABDRABOU A (2016) Celiac trunk and hepatic artery variants: A retrospective preliminary MSCT report among Egyptian patients. Egypt J Radiol Nucl Med, 47: 1451-1458.
PANAGOULI E, VENIERATOS D, LOLIS E, SKANDALAKIS P (2013) Variations in the anatomy of the celiac trunk: A systematic review and clinical implications. Ann Anat, 195: 501-511.
PINEDA M, FIGUEROA V, CASTILLO S, ANDA M, PRADEL A, LEÓN E, MENDIZÁBAL A (2019) Morfometría y variantes anatómicas del tronco celíaco en población mexicana. Int J Morphol, 37: 174-177.
ROSSI EC (1904) Studio morfologico delle arterie dello stomaco. Arch Ital Anat Embryol, 255: 278-288.
SEHGAL G, SRIVASTAVA AK, SHARMA PK, KUMAR N, SINGH R, PARIHAR A, AGA P (2013) Morphometry of the celiac trunk: A multidetector computed tomographic angiographic study. J Anat Soc India, 62: 23-27.
SONG SY, CHUNG JW, YIN YH, JAE HJ, KIM HC, JEON UB, CHO BH, SO YH, PARK JH (2010) Celiac axis and common hepatic artery variations in 5002 patients: Systematic analysis with spiral CT and DSA. Radiology, 255: 278-288.
TANDLER J (1904) Über die Varietäten der Arteria coeliaca und deren Entwicklung. Beiträge Ref Anat Entwicklungsgesch, 25: 473-500.
VANDAMME JPJ, BONTE J (1985) The branches of the celiac trunk. Cells Tissues Organs, 122: 110-114.
VENARA A, PITTET O, LU TL, DEMARTINES N, HALKIC N (2013) Aberrant right hepatic artery with a prepancreatic course visualized prior to pancreaticoduodenectomy. J Gastrointest Surg, 17: 1024-1026.
VON HALLER A (1756) Icones Anatomicae Quibus Praecipuae Aliquae Partes Corporis Humani Delineatae Proponuntur & Arteriarum Potissimum Historia. Göttingen.
WINSTON CB, LEE NA, JARNAGIN WR, TEITCHER J, DEMATTEO RP, FONG Y, BLUMGART LH (2007) CT angiography for delineation of celiac and superior mesenteric artery variants in patients undergoing hepatobiliary and pancreatic surgery. Am J Roentgenol, 189: 123.
WINTER TC, NGHIEM HV, FREENY PC, HOMMEYER SC, MACK LA (1995) Hepatic arterial anatomy: demonstration of normal supply and vascular variants with three-dimensional CT angiography. Radiographics, 15: 771-780.