The present study was designed to assess the incidence of different anatomical variations of the left coronary artery (LCA) and their branches. Also, it was designed to study the dominance pattern of coronary arteries. It was carried out on 30 human adult cadaveric hearts, 200 three-dimensional coronary computed tomographic angiography (3D-CCTA) scans, and 200 coronary catheterization angiography obtained from the Anatomy, Radiology, and Cardiology Department, Beni-Suef, Cairo as well as El Minia University. The current work revealed that there was not any case of higher take-off origin of the left coronary artery. The incidence of the LCA branching mode was 74.1%, 24.18%, and 0.46% for the bifurcation, trifurcation, and tetrafurcation, respectively. A statistically significant correlation between the diagonal branches of the left anterior descending artery and the mode of branching of the LCA had been demonstrated. The incidence of coronary artery dominance was 77%, 14%, and 9% for right, left, and co-dominant pattern. It can be concluded that perfect knowledge of the anatomical variations of the mode of branching of the LCA is essential for cardiologists and radiologists, during diagnostic and therapeutic cardiac procedures.


 Fig. 1.- A dissected human heart. A: bifurcation pattern of the left coronary artery (LCA) into the left anterior descending (LAD) and circumflex (CX) arteries. The LAD artery gives a diagonal (D) branch and the CX gives an obtuse marginal (OM) branch. Note: AO is referred to as ascending aorta and NA is referred to as a sinoatrial nodal branch of the left coronary artery. B: trifurcation pattern of the left coronary artery (LCA) into the left anterior descending artery (LAD), one ramus intermedius (RI), and circumflex artery (CX) branches. The RI artery appears equal in size to the LAD and gives muscular branches (M) to the left ventricle. C: left coronary artery (LCA) dividing into four branches (tetrafurcation): left anterior descending (LAD), circumflex (CX) and two ramus intermedius (RI) arteries. D: left coronary artery (LCA) dividing into two branches: left anterior descending (LAD) and circumflex (CX). Myocardial bridge (M.B.) interrupting the course of LAD is also observed.
Fig. 1.- A dissected human heart. A: bifurcation pattern of the left coronary artery (LCA) into the left anterior descending (LAD) and circumflex (CX) arteries. The LAD artery gives a diagonal (D) branch and the CX gives an obtuse marginal (OM) branch. Note: AO is referred to as ascending aorta and NA is referred to as a sinoatrial nodal branch of the left coronary artery. B: trifurcation pattern of the left coronary artery (LCA) into the left anterior descending artery (LAD), one ramus intermedius (RI), and circumflex artery (CX) branches. The RI artery appears equal in size to the LAD and gives muscular branches (M) to the left ventricle. C: left coronary artery (LCA) dividing into four branches (tetrafurcation): left anterior descending (LAD), circumflex (CX) and two ramus intermedius (RI) arteries. D: left coronary artery (LCA) dividing into two branches: left anterior descending (LAD) and circumflex (CX). Myocardial bridge (M.B.) interrupting the course of LAD is also observed.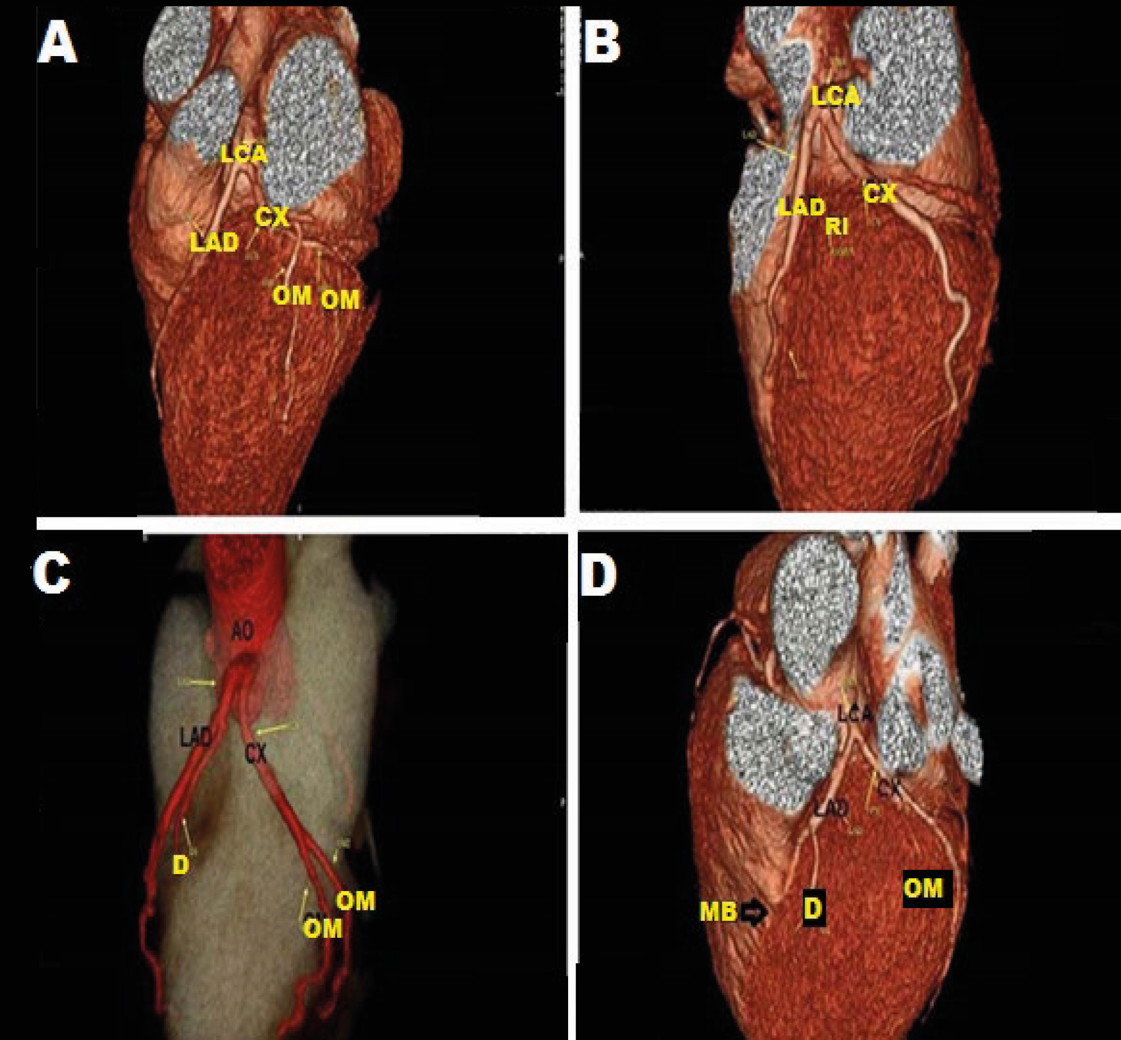 Fig. 2.- 3D CT coronary angiography. A: The left coronary artery (LCA) dividing into left anterior descending (LAD) and circumflex (CX) arteries. Two obtuse marginal (OM) arteries are branches of CX. B: The left coronary artery (LCA) dividing into left anterior descending (LAD) and circumflex (CX) arteries. A diagonal branch (D) is seen arisen from LAD and obtuse marginal (OM) is seen arise from CX. C: The left anterior descending (LAD) and circumflex (CX) arteries are arising directly from the ascending aorta (AO) by a separate ostium and the left coronary artery (LCA) is absent. A diagonal branch (D) is seen arisen from LAD and obtuse marginal (OM) is seen arise from CX. D: The left coronary artery (LCA) dividing into left anterior descending (LAD) and circumflex (CX) arteries. A diagonal branch (D) is seen arisen from LAD and obtuse marginal (OM) is seen arise from CX. Myocardial bridge (M.B.) interrupting the course of LAD is also observed.
Fig. 2.- 3D CT coronary angiography. A: The left coronary artery (LCA) dividing into left anterior descending (LAD) and circumflex (CX) arteries. Two obtuse marginal (OM) arteries are branches of CX. B: The left coronary artery (LCA) dividing into left anterior descending (LAD) and circumflex (CX) arteries. A diagonal branch (D) is seen arisen from LAD and obtuse marginal (OM) is seen arise from CX. C: The left anterior descending (LAD) and circumflex (CX) arteries are arising directly from the ascending aorta (AO) by a separate ostium and the left coronary artery (LCA) is absent. A diagonal branch (D) is seen arisen from LAD and obtuse marginal (OM) is seen arise from CX. D: The left coronary artery (LCA) dividing into left anterior descending (LAD) and circumflex (CX) arteries. A diagonal branch (D) is seen arisen from LAD and obtuse marginal (OM) is seen arise from CX. Myocardial bridge (M.B.) interrupting the course of LAD is also observed.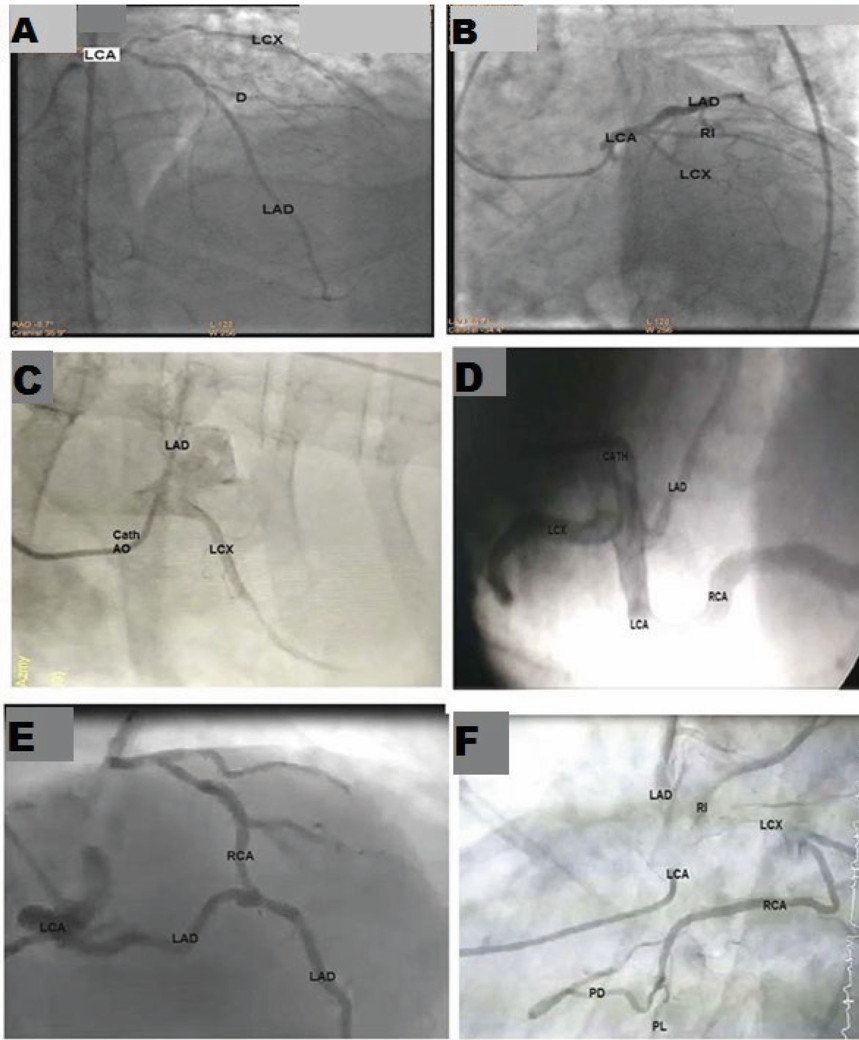 Fig. 3.- Coronary catheterization angiography study showing: A: The left coronary artery (LCA) dividing into left anterior descending (LAD) and circumflex (LCX) arteries (bifurcation). One diagonal (D) is seen as a branch of LAD. B: The left coronary artery (LCA) dividing into 3 branches: left anterior descending (LAD), circumflex (LCX), and ramus intermedius (RI) arteries (Trifurcation). C: Absent left coronary artery (LCA). As left anterior descending (LAD) and left circumflex (LCX) arteries arise from separate ostium from the aorta. D: The left coronary artery (LCA) is dividing into left anterior descending (LAD) and left circumflex (LCX) arteries and also gives rise to the right coronary artery (RCA) from its beginning. E: The left coronary artery (LCA) is dividing into left anterior descending (LAD) and left circumflex (LCX) arteries. The right coronary artery (RCA) is raised from LAD. F: The left coronary artery (LCA) is dividing into left anterior descending (LAD), left circumflex (LCX), and ramus intermedius (RI) arteries. RCA is raised from LCX. RCA is terminated into two terminal branches (PL and PD).
Fig. 3.- Coronary catheterization angiography study showing: A: The left coronary artery (LCA) dividing into left anterior descending (LAD) and circumflex (LCX) arteries (bifurcation). One diagonal (D) is seen as a branch of LAD. B: The left coronary artery (LCA) dividing into 3 branches: left anterior descending (LAD), circumflex (LCX), and ramus intermedius (RI) arteries (Trifurcation). C: Absent left coronary artery (LCA). As left anterior descending (LAD) and left circumflex (LCX) arteries arise from separate ostium from the aorta. D: The left coronary artery (LCA) is dividing into left anterior descending (LAD) and left circumflex (LCX) arteries and also gives rise to the right coronary artery (RCA) from its beginning. E: The left coronary artery (LCA) is dividing into left anterior descending (LAD) and left circumflex (LCX) arteries. The right coronary artery (RCA) is raised from LAD. F: The left coronary artery (LCA) is dividing into left anterior descending (LAD), left circumflex (LCX), and ramus intermedius (RI) arteries. RCA is raised from LCX. RCA is terminated into two terminal branches (PL and PD).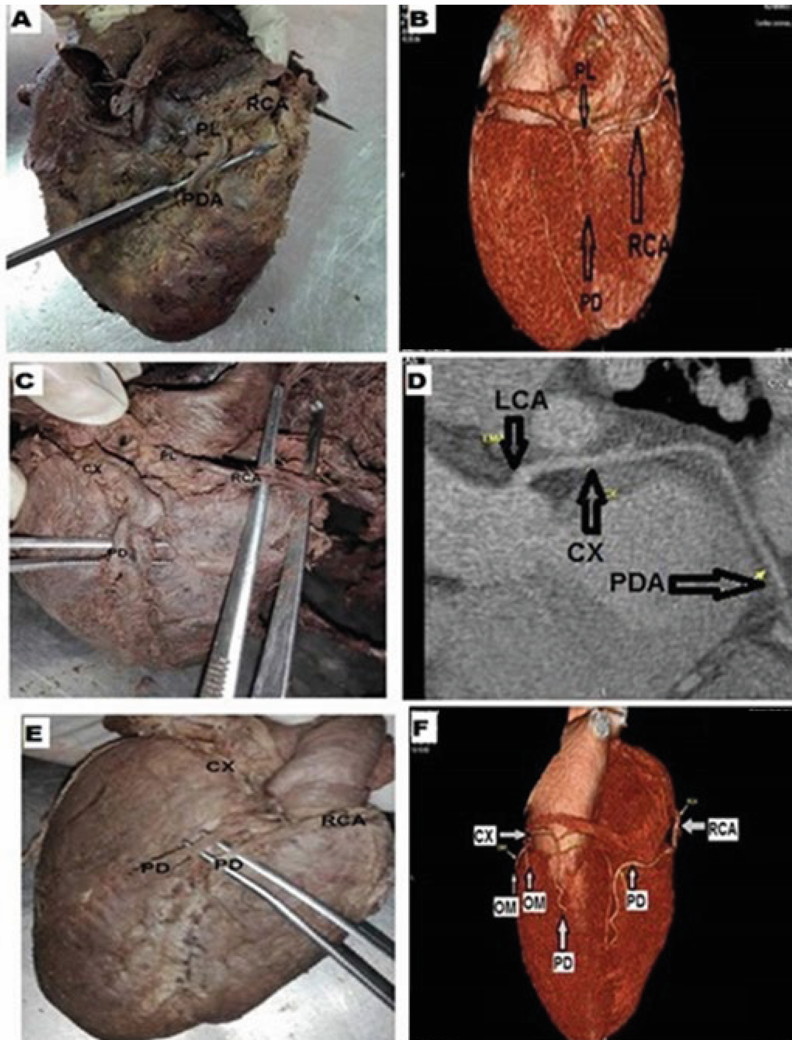 Fig. 4.- Pictures of A: Cadaver dissection and B: 3D CT angiography. Both of them showing the right coronary artery (RCA) termination into a posterior descending artery (PDA) and posterolateral artery (PL) in the right dominant heart. C: Cadaver dissection and D: 3D CT angiography showing a left dominance pattern where the posterior descending artery (PD) arose from the circumflex artery (CX), not from the right coronary artery (RCA). RCA is terminated by giving the posterolateral artery (PL). E: Cadaver dissection and F: 3D CT angiography showing a balanced pattern where the posterior descending artery (PD) arises from both the right coronary artery (RCA) and circumflex artery (CX), and both PD lying within the posterior interventricular sulcus.
Fig. 4.- Pictures of A: Cadaver dissection and B: 3D CT angiography. Both of them showing the right coronary artery (RCA) termination into a posterior descending artery (PDA) and posterolateral artery (PL) in the right dominant heart. C: Cadaver dissection and D: 3D CT angiography showing a left dominance pattern where the posterior descending artery (PD) arose from the circumflex artery (CX), not from the right coronary artery (RCA). RCA is terminated by giving the posterolateral artery (PL). E: Cadaver dissection and F: 3D CT angiography showing a balanced pattern where the posterior descending artery (PD) arises from both the right coronary artery (RCA) and circumflex artery (CX), and both PD lying within the posterior interventricular sulcus.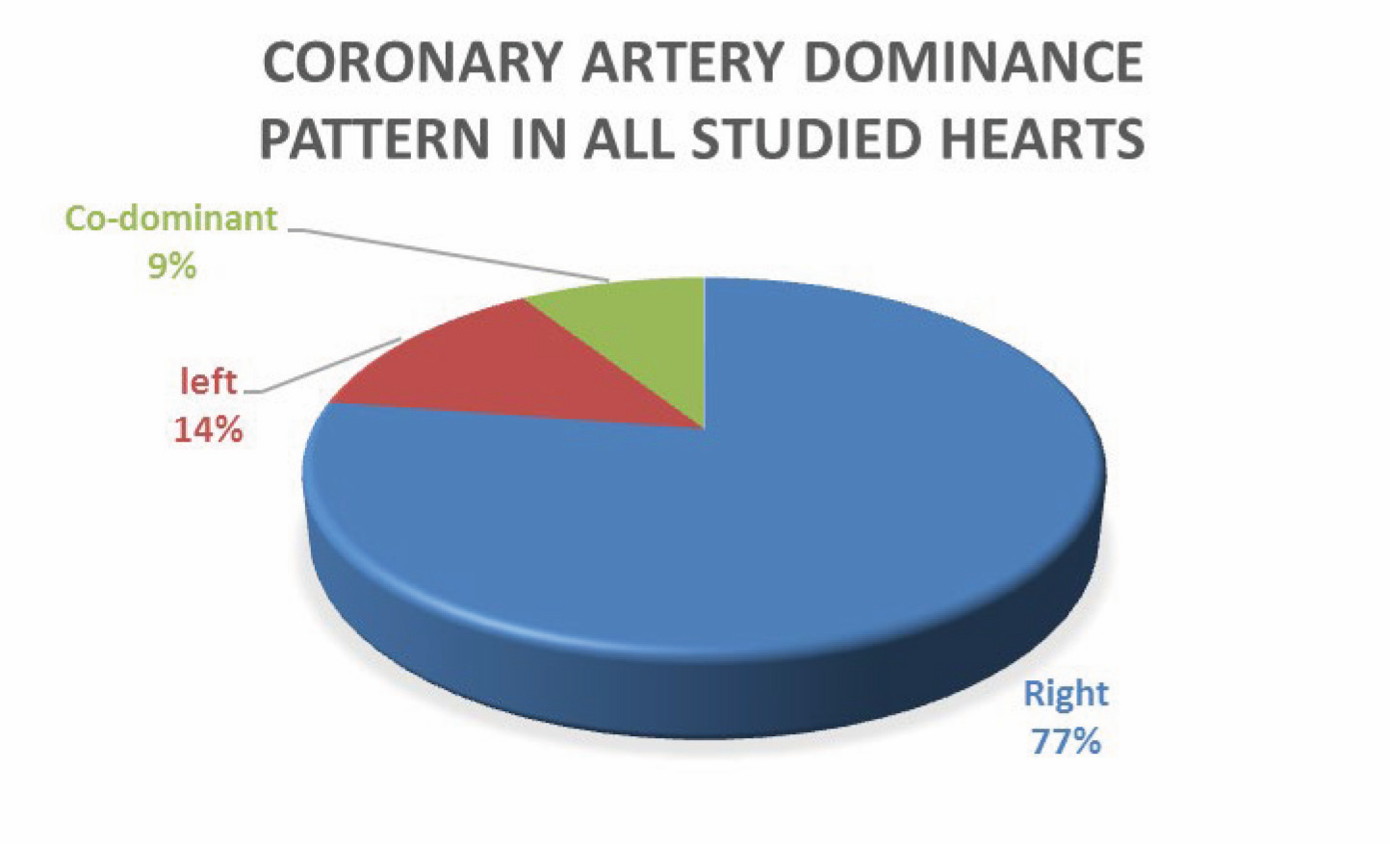 Fig. 5.- A pie chart demonstrating the coronary artery dominance pattern in all studied hearts.
Fig. 5.- A pie chart demonstrating the coronary artery dominance pattern in all studied hearts.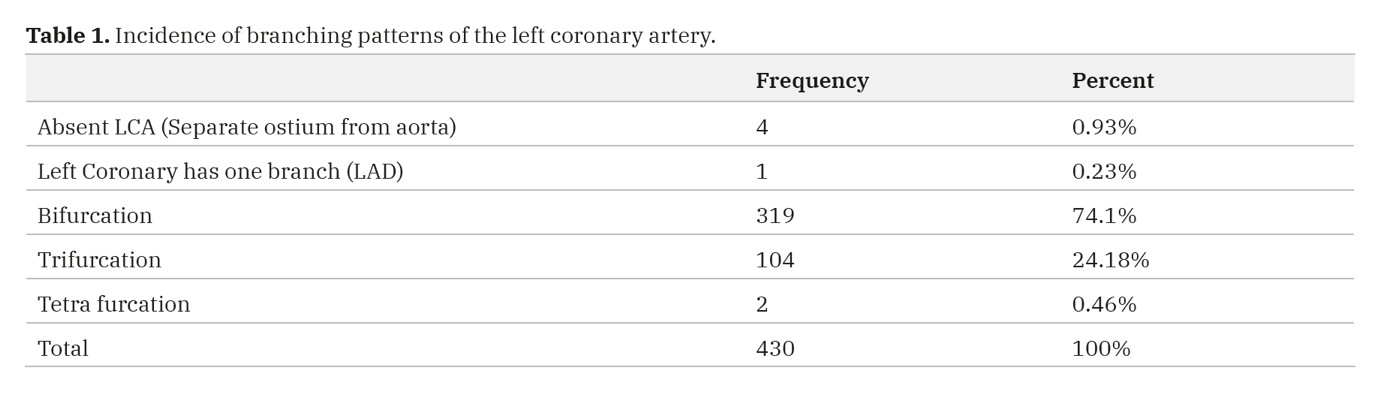 Table 1. Incidence of branching patterns of the left coronary artery.
Table 1. Incidence of branching patterns of the left coronary artery. 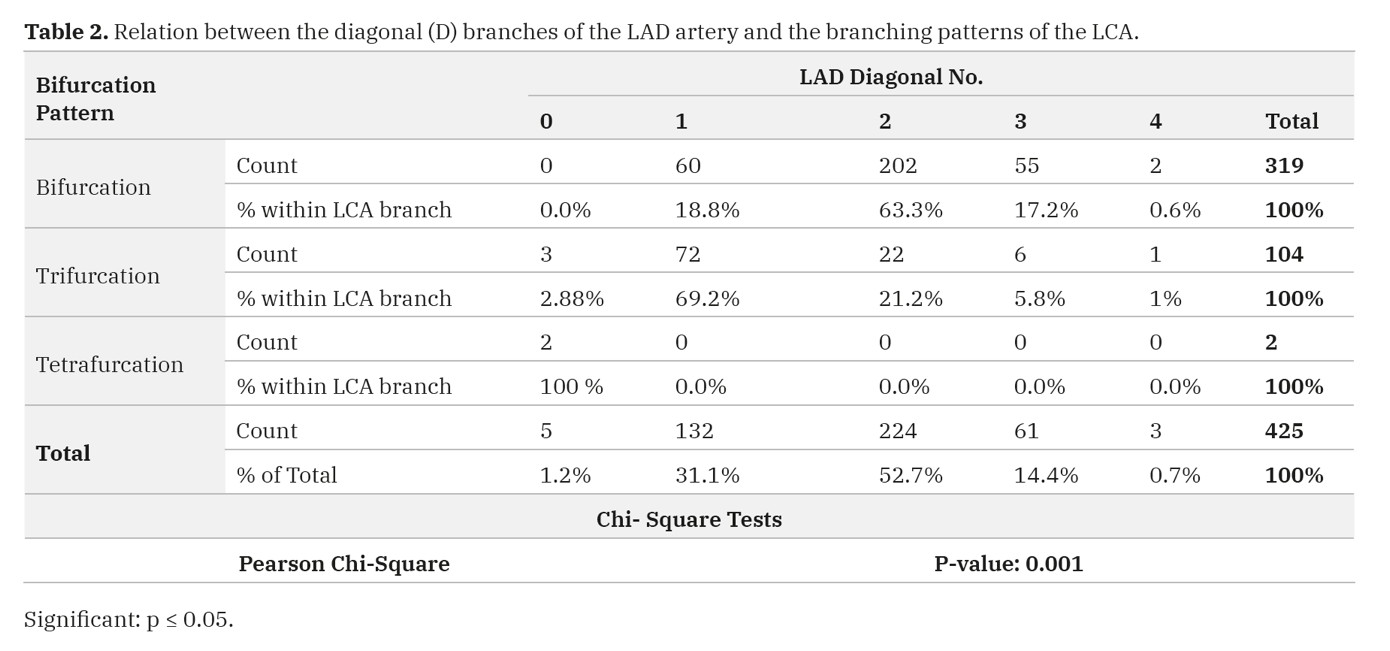 Table 2. Relation between the diagonal (D) branches of the LAD artery and the branching patterns of the LCA.
Table 2. Relation between the diagonal (D) branches of the LAD artery and the branching patterns of the LCA. Table 3. Relation between the incidence of the myocardial bridges and the branching patterns of the LCA.
Table 3. Relation between the incidence of the myocardial bridges and the branching patterns of the LCA.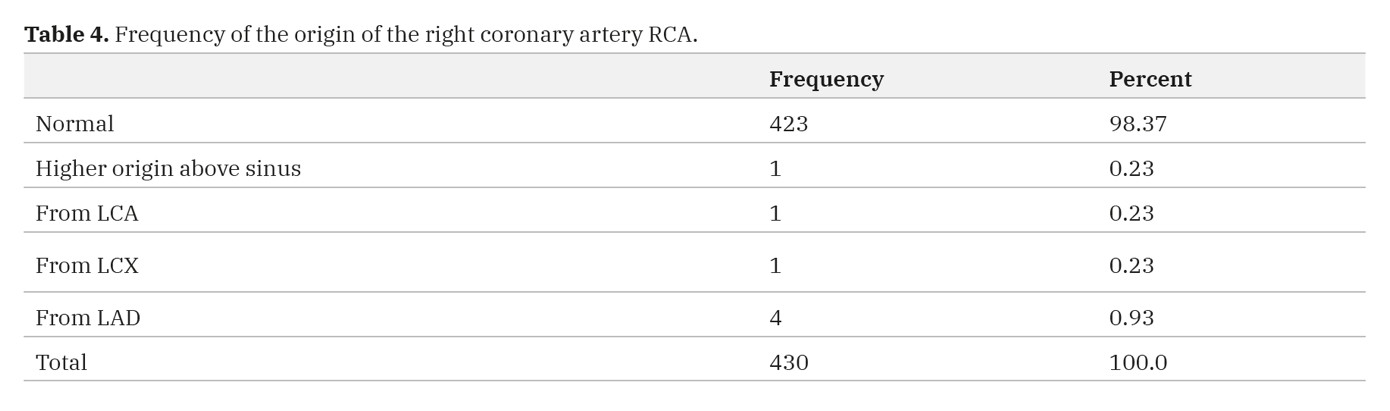 Table 4. Frequency of the origin of the right coronary artery RCA.
Table 4. Frequency of the origin of the right coronary artery RCA.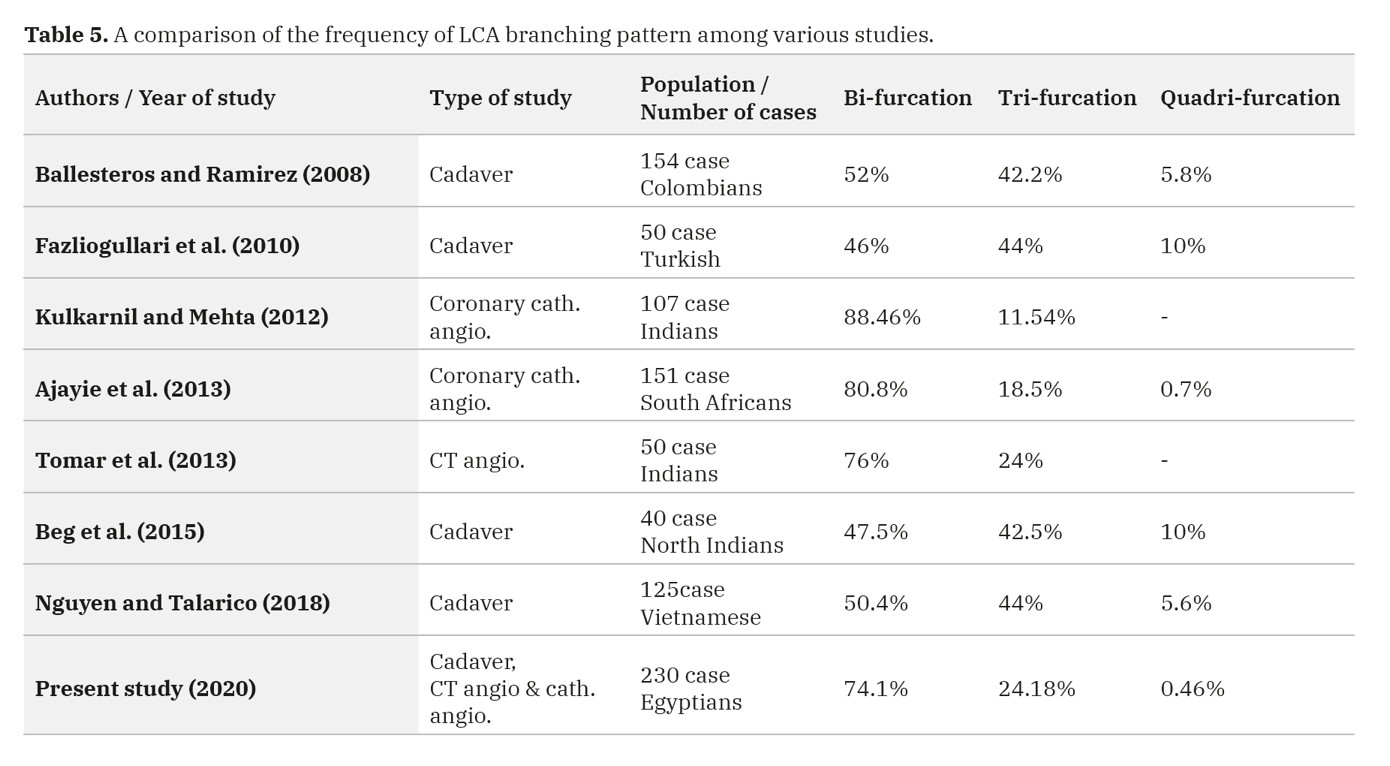 Table 5. A comparison of the frequency of LCA branching pattern among various studies.
Table 5. A comparison of the frequency of LCA branching pattern among various studies.